Download
1 / 26
260 likes | 447 Views
The Molecular face of red cells. Designer genes. What is it?. Refers to the detection of the molecular basis of an antigen rather than the antigen itself Prerequisites: Knowledge of the molecular structure Appropriate genotyping methods. A buzzzzz word??. Is there a need?

E N D
The Molecular face of red cells Designer genes
What is it? • Refers to the detection of the molecular basis of an antigen rather than the antigen itself • Prerequisites: • Knowledge of the molecular structure • Appropriate genotyping methods
A buzzzzz word?? • Is there a need? • What are the potential advantages? • Is it sustainable? • Service / research mode?
Some real life scenarios • 25 year old - aplastic anemia • O pos few years ago – transfused 25 units of red cells / PRCs etc • Now requires a transfusion
New sample for crossmatch • O Rh Negative • Done on 3 different platforms, using different antisera • History – No transplant
Patient is convinced we have gooooofed – wants an explanation
Request from OG • 27 year old • 4th pregnancy at 10 weeks of gestation • 1 miscarriage, 2 deaths with severe hydrops • Blood group – O Rh negative, ICT , antibody screen Pos. Anti D – titre 1:256
A question……. • What will the fate of this pregnancy be ?
Indications for DNA typing • Fetal DNA analysis • Typing multiply transfused • Serological discrepancies – weak D / ABO Subgroups / AIHA with pos DAT …… • QC of antibody screening /ID RBCs • Routine phenotyping of red cells
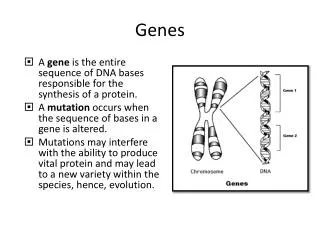
RBC Antigens • Products of Genes • Antigens carried by proteins – direct products of genes- Rh / Kell • Antigens carried by Carbohydrates – under the control of genes coding for the glycosyltransferases – ABO / H
Nature of differences • Mostly SNPs • Single amino acid differences
However………. • Multiple alleles can code for a single same antigen!!!!! • Events other than SNPs in the same region – can affect antigen expression • Hence incomplete genotyping may not correlate with phenotyping
The D antigen • Greatest Contribution to health care – in pregnancy • To assess if a D negative Mother is carrying a D positive baby • If mother unsensitised – Anti D given only if baby is Rh positive • If mother sensitised – impact on clinical follow up
Fetal DNA in maternal serum • Previously fetal DNA testing done on Amniocentesis samples • Now - found that sufficient amount of fetal DNA is present in sera of mothers • About 3-10% of free plasma DNA in pregnant mothers is fetal. Clears rapidly post pregnancy
Cell free fetal DNA • Occurs due to apoptosis and necrosis etc of placental tissue • Part of a process of physiological remodelling • Results in ffDNA getting released into maternal plasma
From when? • 1st trimester • Average 17 weeks
When can it be done? • Akolekar et al – 11 – 13 weeks of pregnancy • High throughput robotic technique • 100% pos predictive value • 96.5% negative predictive value • Cardo et al - sensitivity of 100% and a specificity of 93%, with a 97% diagnostic accuracy for RhD genotyping • first trimester of pregnancy • using a quantitative PCR
Sensitivity ----- • Compared to post natal serology • Muller et al – 2008 • >1000 typings • 25 weeks of pregnancy • >99.6% concordance
Platforms available • Real time PCR • The luminex platform • Automated High throughput analysers using these technologies available • Blood chip technology
The Multiply transfused • Cannot be typed by serology – mixed field reaction seen • DNA from WBC – Accurate type • Epithelia also can be used • Helps select blood for transfusion
Multiply transfused - contd • Likely to be sensitised • Worth antigen matching • If sensitised – can attempt to antigen match henceforth – to prevent further sensitisation