Download
1 / 1
10 likes | 155 Views
OPTIONAL LOGO HERE. Laparoscopic assisted vaginal hysterectomy in a District General Hospital- Audit of clinical practice M Ahmad, K Agarwal , Mr K Farag , Barnsley Hospital NHS Foundation Trust. OPTIONAL LOGO HERE. OBJECTIVE. RESULTS. RESULTS. CONCLUSION.

E N D
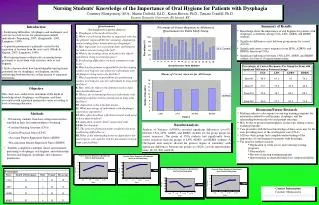
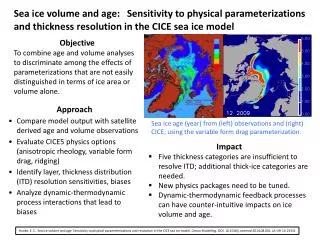
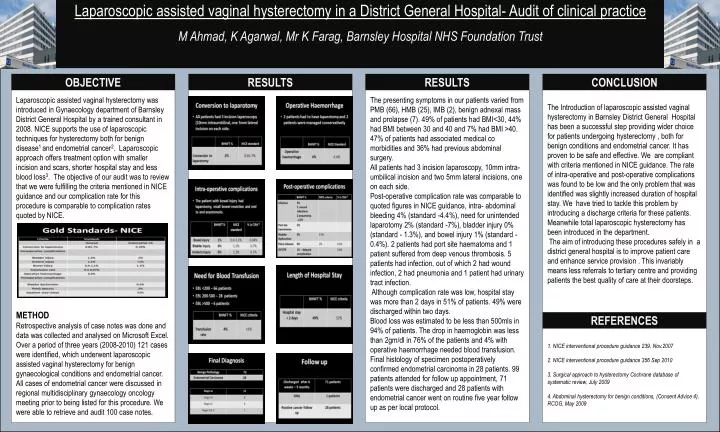
OPTIONALLOGO HERE Laparoscopic assisted vaginal hysterectomy in a District General Hospital- Audit of clinical practice M Ahmad, K Agarwal, Mr K Farag, Barnsley Hospital NHS Foundation Trust OPTIONALLOGO HERE OBJECTIVE RESULTS RESULTS CONCLUSION The presenting symptoms in our patients varied from PMB (66), HMB (25), IMB (2), benign adnexal mass and prolapse (7). 49% of patients had BMI<30, 44% had BMI between 30 and 40 and 7% had BMI >40. 47% of patients had associated medical co morbidities and 36% had previous abdominal surgery. All patients had 3 incision laparoscopy, 10mm intra-umbilical incision and two 5mm lateral incisions, one on each side. Post-operative complication rate was comparable to quoted figures in NICE guidance, intra- abdominal bleeding 4% (standard -4.4%), need for unintended laparotomy 2% (standard -7%), bladder injury 0% (standard - 1.3%), and bowel injury 1% (standard - 0.4%). 2 patients had port site haematoma and 1 patient suffered from deep venous thrombosis. 5 patients had infection, out of which 2 had wound infection, 2 had pneumonia and 1 patient had urinary tract infection. Although complication rate was low, hospital stay was more than 2 days in 51% of patients. 49% were discharged within two days. Blood loss was estimated to be less than 500mls in 94% of patients. The drop in haemoglobin was less than 2gm/dl in 76% of the patients and 4% with operative haemorrhage needed blood transfusion. Final histology of specimen postoperatively confirmed endometrial carcinoma in 28 patients. 99 patients attended for follow up appointment, 71 patients were discharged and 28 patients with endometrial cancer went on routine five year follow up as per local protocol. Laparoscopic assisted vaginal hysterectomy was introduced in Gynaecology department of Barnsley District General Hospital by a trained consultant in 2008. NICE supports the use of laparoscopic techniques for hysterectomy both for benign disease1 and endometrial cancer2. Laparoscopic approach offers treatment option with smaller incision and scars, shorter hospital stay and less blood loss3. The objective of our audit was to review that we were fulfilling the criteria mentioned in NICE guidance and our complication rate for this procedure is comparable to complication rates quoted by NICE. METHOD Retrospective analysis of case notes was done and data was collected and analysed on Microsoft Excel. Over a period of three years (2008-2010) 121 cases were identified, which underwent laparoscopic assisted vaginal hysterectomy for benign gynaecological conditions and endometrial cancer. All cases of endometrial cancer were discussed in regional multidisciplinary gynaecology oncology meeting prior to being listed for this procedure. We were able to retrieve and audit 100 case notes. The Introduction of laparoscopic assisted vaginal hysterectomy in Barnsley District General Hospital has been a successful step providing wider choice for patients undergoing hysterectomy , both for benign conditions and endometrial cancer. It has proven to be safe and effective. We are compliant with criteria mentioned in NICE guidance. The rate of intra-operative and post-operative complications was found to be low and the only problem that was identified was slightly increased duration of hospital stay. We have tried to tackle this problem by introducing a discharge criteria for these patients. Meanwhile total laparoscopic hysterectomy has been introduced in the department. The aim of introducing these procedures safely in a district general hospital is to improve patient care and enhance service provision . This invariably means less referrals to tertiary centre and providing patients the best quality of care at their doorsteps. REFERENCES 1. NICE interventional procedure guidance 239, Nov.2007 2. NICE interventional procedure guidance 356 Sep 2010 3. Surgical approach to hysterectomy Cochrane database of systematic review, July 2009 4. Abdominal hysterectomy for benign conditions, (Consent Advice 4), RCOG, May 2009