Download
1 / 26
260 likes | 465 Views
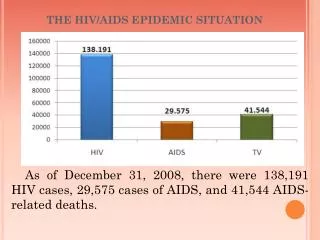
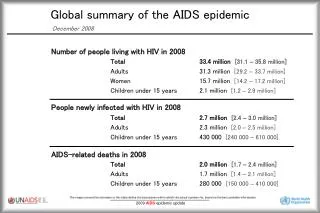
THE HIV EPIDEMICS IN SUB-SAHARAN AFRICA: THE PAST AND THE FUTURE. Anne Buvé Institute of Tropical Medicine, Antwerp. UNAIDS REPORT ON THE GLOBAL AIDS EPIDEMIC, 2010. Adults & children with HIV in 2009 33.3 million In sub- Saharan Africa 22.5 million

E N D
THE HIV EPIDEMICS IN SUB-SAHARAN AFRICA: THE PAST AND THE FUTURE.Anne BuvéInstitute of Tropical Medicine, Antwerp
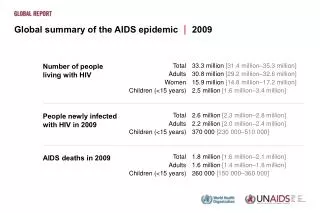
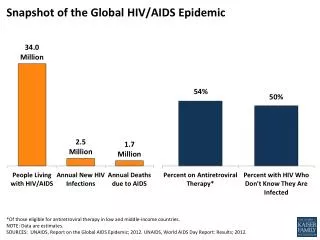
UNAIDS REPORT ON THEGLOBAL AIDS EPIDEMIC, 2010 • Adults & childrenwith HIV in 2009 33.3 million • In sub-SaharanAfrica22.5 million • New HIV infections in 2009 2.6 million • In sub-SaharanAfrica1.8 million Twothirds of allinfections worldwide are in sub-SaharanAfrica
THE ORIGINS OF HIV • 1981: first clinicaldescrition of AIDS in gay men in Los Angeles • The oldestknown case of HIV infection is in a man wholived in Kinshasa in 1959 • Estimated date of introduction of HIV-1 and HIV-2 in human population HIV-1: 1880 (?) / 1920 - 1930 HIV-2: 1930 – 1945
Sooty mangabeysin West Africa: • SIVsm VIH-2 • Chimpanzees in Central Africa: • SIVcpz VIH-1(group M)
HOW DID THE TRANSMISSION OCCUR? • Most likely route of transmission through handling of infectedbushmeat • Question: howcouldthisevolveto a pandemic?
HYPOTHESES De Sousa JD, Müller V, Lemey Ph, Vandamme A. High GUD incidence in the early 20th centurycreated a particularlypermissive time windowfor the originandinitial spread of epidemic HIV strains. PlosOne 2010; 5(4): e9936
KINSHASA IN THE 1920’s (then Leopoldville) • One of the largest cities in Central Africa and fast growing • High male:female ratio (4:1) and floursihing commercial sex work • In the 1920’s epidemics of syphilis with high rates of GUD and high transmission of HIV • According to J. Pépin: also frequent use of injections
A global view of HIV infection 33.3 million people living with HIV, 2009 2.2
THE MULTICENTRE STUDY ON FACTORS DETERMINING THE DIFFERENTIAL SPREAD OF HIV IN 4 AFRICAN CITIES
MAIN RESULTS • Differences in sexualbehaviourbetween the 4 cities BUT no patternthatcouldexplain the differences in HIV • Twobiological factors appearedtodetermine the differences in HIV spread • Male circumcision: protective - prevalent in Cotonou and Yaoundé • HSV-2 infection – more prevalent in KisumuandNdola
HSV-2 PREVALENCE BY AGE AND CITY Females Males % HSV-2 seropositive Age Kisumu Yaounde Ndola Cotonou
RISK OF HIV IN HSV-2 POSITIVE WOMEN & MEN: META-ANALYSIS OF LONGITUDINAL STUDIES(Glynn et al, AIDS 2009; 23: 1595-1598) Summary OR Womengeneral pop. 3.4 (2.4 – 4.8) Heterosexual men 2.8 (2.1 – 3.7)
POSSIBLE IMPACT OF CONTROL OF HSV-2 IN AFRICA • Women • HSV-2 prevalence 29-71% • 38%- 60% of new HIV infections in women could be attributable to HSV-2 • Men • HSV-2 prevalence 5-53% • 8%- 49% of new HIV infections in men could be attributable to HSV-2
INTERVENTIONS TO DECREASE INCIDENCE AND PREVALENCE OF HSV-2? • Trials of supressive therapy with acyclovir / valacyclovir • No effect on risk of HIV acquisition • No effect on risk of onward transmission of HIV in discordant couples • Vaccine? • Tenofovir gel?
MALE CIRCUMCISION CONFIRMED TO BE PROTECTIVE IN 3 RCT’s • 3 RCT’sdemonstratedprotective effect of about60%
ANTIRETROVIRAL DRUGS IN HIV PREVENTION • Topical antiretrovirals: microbicides • Oral antiretrovirals: PrEP in HIV- • Treatment of HIV infected persons
PrEP: Tenofovir or Truvada (TDF+emcitrabine) • MSM (iPrEX) Americas, S Africa, Thailand • Women (FEM-PrEP) Kenya, Tanzania, S Africa • Heterosexualmen&womenBotswana • Discordant couples Kenya, Uganda Protective effect 44% Stopped (futility) 63% 73%
TREATMENT OF INFECTED PERSONS: HPTN05 Discordant couples • Start treatment of the infected partner at CD4 count 350-550 versus • Start treatment at CD4 count < 250) Efficacy in preventing transmission: 96%
A GLIMPSE OF THE FUTURE: HIV IN YOUNG PEOPLE Population based studies 2004-2007 • Prevalence in women aged 15-24 years > 15% • Botswana, Lesotho, Swaziland, South Africa > 10% • Zimbabwe < 10% • Zambia, Malawi
GOOD NEWS: RECENT TRENDS • Population based studies - women 15-24 years: decrease in Zambia and Zimbabwe • Young antenatal clinic attenders (<25 years): decrease in Botswana*, Lesotho, Malawi*, Namibia, Swaziland, Zimbabwe* and Zambia Statistically significant Gouws et al. AIDS 2008; suppl 4: S5-S16
TRENDS IN KISUMU: 1996 – 2006/2008 • Young women 15-24 years 1996: 30% 2006: 16% • Female sex workers 1996: 75%condom use: 50% 2008: 58%condom use: 75%