Download
1 / 13
170 likes | 929 Views
Coronary Artery Calcification. & Computed Tomography Scoring. Coronary Artery Disease (CAD). CAD is the end result of the accumulation of atheromatous plaques in the walls of the coronary arteries. CAD is the leading cause of death in the world.

E N D
Coronary Artery Calcification & Computed Tomography Scoring
Coronary Artery Disease (CAD) • CAD is the end result of the accumulation of atheromatous plaques in the walls of the coronary arteries. • CAD is the leading cause of death in the world. • CAD presents as a myocardial infarction (MI) or sudden cardiac death in ~50% of individuals with the pathology. • CAD is conventionally screened for by office-based risk screening methods, such as the Framingham Risk Score (FRS) in the US or the Prospective Cardiovascular Münster (PROCAM) study in Germany. • These screens only predict 60-65% of cardiovascular risk, not detecting many individuals who do not have traditional risk factors.
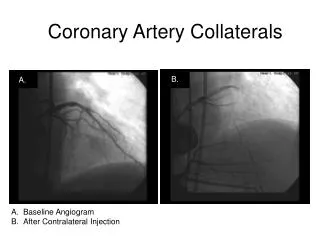
Coronary Atherosclerosis • Atherosclerosis describes a chronic inflammatory process in arterial walls. • Associated with deposition of cholesterol by LDL without adequate removal by HDL. • Chronic atherosclerosis may lead to: • Stenosis and claudication • Plaque rupture and thrombosis • Long-standing association between arterial disease and calcification. • Calcification ≈ atherosclerosis • Furthermore, there is association between the presence of coronary calcification and risk of cardiovascular events.
Electron Beam and Multidetector CT Problems imaging the heart: • Heart is beating (we hope!) • Beats are fast movements • Coronary arteries move a distance of several times their diameter each beat Electron Beam CT (EBCT) • Differs from conventional (helical/spiral) CT in that X-ray source is not rotated around patient • Obtains slices very quickly Multidetector CT (MDCT) • Much more widely available • Most coronary calcium studies use this • Multiple detectors allow increased imaging speed • Some detectors use EKG-gating to image diastole only (so coronary arteries are full) CT = Computed Tomography
The Test Procedure • No special preparation, nor medication restrictions. • Patient lies in CT scanner for about 10 minutes and must hold breath between 10-30 seconds during imaging. • Radiation exposure: 0.7-3.0 mSv (milli-Sieverts) • Avg. yearly “natural” background exposure in US: 3 mSv • Diagnostic cardiac catheterization: 4.5 mSv • Coronary Artery Calcification (CAC) Score – Agatston Score • Based on area and density of calcified plaques • Typical report includes: • Agatston score for each major coronary artery • Total Agatston score for the patient • Several representative images
CAC Scoring • In multiple studies the following definitions have been used to correlate the CAC score and the coronary plaque burden: • 0 No identifiable disease • 1 – 99 Mild Disease • 100 – 399 Moderate Disease • >400 Severe Disease
Representative Images • On CT, calcium has high attenuation values very bright! LCA
Framingham Models • All adults should undergo an office-based assessment as an initial step to identify patients at higher-risk for a coronary event. • Risk Categories of the Framingham Models: • Defines risk of a cardiac event over 10 years. • Low: < 10% • Intermediate: 10-20% • High: > 20% • Framingham scores are population-based, and do not take into account an individual’s actual burden of atherosclerotic disease. • The majority of all cardiac events occurs in the intermediate risk cohort, yet treating all these individuals is cost-inefficient. • Therefore, CAC testing may detect those individuals in this risk group who actually have coronary atherosclerosis, and who would benefit from more aggressive therapy.
CAC and Obstructive Disease • CAC testing has a high sensitivity and high negative predictive value (NPV = 98%) for obstructive coronary artery disease (CAD), but limited specificity. • Therefore, CAC testing can be used to rule out angiographically significant CAD in symptomatic patients. • CAC could be used as a filter before catheterization – patients with a negative CAC would not continue to the cath lab. • This could save unnecessary catheterization procedures in patients presenting to the ED with chest pain. • In another scenario, a low CAC score precludes the need for a myocardial perfusion SPECT (MPS), since the probability of an abnormal scan would be extremely low. • Remember though, a positive CAC indicates atherosclerotic disease, and not necessarily obstruction from stenosis. • A person with an elevated CAC score may benefit from further functional testing to detect occult ischemia. • Functional testing is very important to determine the need for revascularization since functionally insignificant lesions do not benefit from revascularization.
CAC Predicts Cardiac Events • CAC is a strong independent predictor of coronary events in both symptomatic and asymptomatic persons. • In a cohort of 10,377 asymptomatic persons followed for an average of 5 years, CAC was an independent predictor of death (p<0.001), with risk increasing proportionally with calcium scores. • A prospective study of 510 type II diabetics showed that CAC scoring predicted cardiovascular events better than the UK Prospective Diabetes Study Risk Score (0.74) and Framingham Score (0.60, p <0.0001) • When added to the Framingham Risk Score, CAC improves the predictive value of death estimation.
Limitations of CAC • Natural history after CAC scoring is unknown. • Heinz Nixdorf Recall Study is currently assessing this, as neither patient, nor physician will be aware of calcium scores. • Multi-Ethnic Study of Atherosclerosis (MESA) will assess long-term outcome of asymptomatic adults who underwent CAC scoring (in addition to other tests) to detect applicability in diffuse ethnic groups. • Unknown effects of intervention based on calcium scoring. • Lipitor appears to improve outcomes when given to patients with baseline score >400, but this was determined retrospectively. • CAC could be useful in determining which patients do not need expensive statin therapy in the short term.
Recommendations • 2007 American College of Cardiology Foundation (ACCF) and the American heart Association (AHA) found that: • CAC screening should not be used in asymptomatic low or high 10-year CHD risk patients according to Framingham criteria. • CAC screening is useful for intermediate 10-year CHD risk (10-20%) according to Framingham criteria. • If the CAC core is elevated (>400), no further testing is indicated at this time. • A low CAC (<100) effectively excludes obstructive CAD in outpatients with atypical chest pain and ER patients with chest pain; however, stress testing is preferred since it gives a clue of exercise capacity. • There is no current evidence that treatment decisions based on CAC scores leads to outcome improvement.
References 1. Budoff MJ, Gul KM: Expert review on coronary calcium. Vasc Health Risk Manag 2008, 4:315-324. 2. Gerber T. UpToDate: Diagnostic and prognostic implications of coronary artery calcification detected by computed tomography. Lasted updated: July 3, 2007. 3. Greenland P, Bonow RO, Brundage BH, Budoff MJ, Eisenberg MJ, Grundy SM, Lauer MS, Post WS, Raggi P, Redberg RF, et al: ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2007, 49:378-402. 4. Kannel WB, Schatzkin A: Sudden death: lessons from subsets in population studies. J Am Coll Cardiol 1985, 5:141B-149B. 5. Kennedy J, Shavelle R, Wang S, Budoff M, Detrano RC: Coronary calcium and standard risk factors in symptomatic patients referred for coronary angiography. Am Heart J 1998, 135:696-702. 6. Rumberger JA, Brundage BH, Rader DJ, Kondos G: Electron beam computed tomographic coronary calcium scanning: a review and guidelines for use in asymptomatic persons. Mayo Clin Proc 1999, 74:243-252.