Download
1 / 20
300 likes | 634 Views
Spontaneous Awakening and Breathing Trials. Brad Winters MD, PhD. March 14, 2013. Spontaneous Awakening and Breathing Trials (SAT &SBT). Spontaneous Awakening and Breathing Trials : VAP Prevention Guidelines. Does not specifically address SAT and SBT, however supports weaning.

E N D
Spontaneous Awakening and Breathing Trials Brad Winters MD, PhD March 14, 2013
Spontaneous Awakening and Breathing Trials : VAP Prevention Guidelines • Does not specifically address SAT and SBT, however supports weaning. • CDC; MMWR Recomm Rep. 2004;53:1-36 • Recommends use of daily interruption or lightening of sedation to avoid constant heavy sedation and to facilitate and accelerate weaning. • Does not specifically address SBT. • ATS/IDSA; AJRCCM 2005;171(4):388-416.
Spontaneous Awakening and Breathing Trials : VAP Prevention Guidelines • Guideline excluded studies that evaluated SAT and SBT. • Canadian VAP Prevention Guidelines; J Crit Care 2008;23(1):138-147. • Recommends the use of combining a daily assessment of readiness wean and daily sedation interruption. • SHEA; ICHE 2008;29:S31-S40.
Spontaneous Awakening Trials Population • Medical ICU patients on mechanical ventilation Intervention(RCT) • Control group: no interruption (N= 68) • Rx group: daily interruption (N= 60) sedation held daily until the patients were awake and could follow instructions or uncomfortable or agitated. • All patients received an infusion of morphine for analgesia. Kress et al. NEJM 2000; 342:1471-77
Spontaneous Awakening Trials Outcomes • 2.4 day reduction duration mechanical ventilation • 33% relative risk reduction • 3.5 day reduction ICU length of stay • 35% relative risk reduction • Hospital length of stay unchanged: control group 16.9 days (8.5-26.6 days) compared to rxgroup 13.3 days (7.3-20.0 days). Kress et al. NEJM 2000; 342:1471-77
Spontaneous Breathing Trials Population • Adult medical and coronary ICU patients on mechanical ventilation (n=300) Intervention (RCT) • Control group: daily screening (RSBI*) (n=151) • Experimental group: daily screening (RSBI) followed by 2-hour SBT (n=149) if they passed the screening test • Physicians were notified when their patients successfully completed the trial of spontaneous breathing. *RSBI: rapid shallow breathing index Ely et al. NEJM 1996; 335:1864-69.
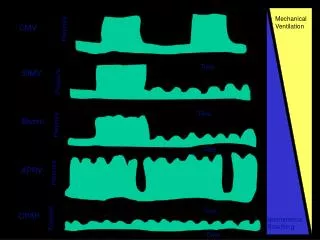
Spontaneous Breathing Trial (SBT) Patient passes SBT safety screen Ventilatorysupport is removed and the patient is allowed to breathe through either a T-tube circuit or a ventilatory circuit using “flow triggering” (rather than triggering by pressure) with a continuous positive airway pressure of 5 cm of water. No changes are required in the fraction of inspired oxygen or the level of positive end-expiratory pressure.
Spontaneous Breathing Trials Outcomes • 1.5 day reduction duration mechanical ventilation • 25% relative risk reduction • 1.0 day reduction ICU length of stay • Not statistically significant • Reductions total ICU costs • Reductions in complications including reintubation Ely et al. NEJM 1996; 335:1864-69.
Treatment protocol Girard et al. Lancet 2008; 371: 126–34
ABC Trial: Awakening and Breathing Controlled trial Population • 336 ICU patients on mechanical ventilation • Four tertiary-care hospitals Intervention(RCT) • Control group: sedation per usual plus daily SBT (n=168) • Rx group: daily SAT followed by SBT (n=168) All patients received an infusion of morphine for analgesia. Girard et al. Lancet 2008; 371: 126–34
ABC Trial: Awakening and Breathing Controlled trial • 3.1 increased days without mechanical ventilation • 21% relative risk increase • 3.8 day reduction ICU length of stay • 29% relative risk reduction • 4.3 day reduction hospital length of stay • 22% relative risk reduction • Number needed to treat (NNT) = 7.4 for one life saved Girard et al. Lancet 2008; 371: 126–34
Practical SAT • The SAT consists of two parts, • a safety screen and • the trial. • The safety screen attempts to assure the trials will not be used when contraindicated. Patients pass the screen unless:
The Safety Screen • Sedation for active seizures or alcohol withdrawal • Already receiving escalating doses of sedative for agitation • Receiving neuromuscular blockers • Active myocardial ischemia in prior 24 hours • Evidence of increased ICP
If patient passes the safetyscreenAwakening Trial • All sedatives and analgesics used for sedation are stopped. Analgesics used for pain are continued. • A patient passes the SAT if awake and can do 3 of 4 simple tasks on request: open eyes, look at caregiver, squeeze hand or stick out their tongue. • OR
If patient passes the safetyscreen • can go ≥ 4 hrs w/o • sustained anxiety • Agitation or pain • RR of 35 for >= 5 minutes • SpO2 < 88% for >=5 minutes • an acute cardiac dysrhythmia • ≥ 2 signs of respiratory distress • Tachycardia, bradycardia, use of accessory muscles, abdominal paradox, diaphoresis, obvious distress
SAT Failure • If a patient fails the SAT, sedatives are restarted at one half the prior dosage and titrated up as needed.
SAT Success? • Maintain adequate oxygenation (SpO2 >=88% on an F1O2 of ≤50% and a PEEP ≤8 cm H2O) • any spontaneous inspiratory effort in a 5-min period • no agitation • no significant use of pressors or inotropes • no evidence of increased ICP
SAT successSBT • Patient breathes through either a T-tube circuit of a ventilatory circuit with CPAP of 5cm H2O or pressure support ventilation of less than 7cm H2O. • Typically FIO2 is ≤50% and PEEP≤8
SBT success? • Patients pass the trial if they don’t develop any of the same criteria as for the SAT for 120m • If they pass, the prescriber is notified for extubation order.