Download
1 / 28

E N D
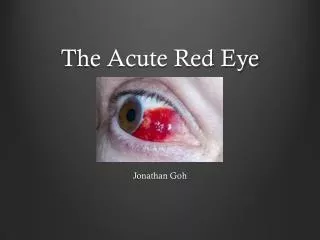
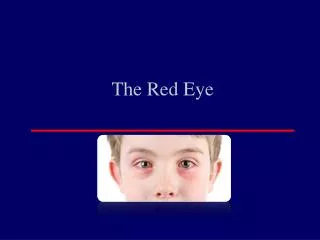
1. The red eye Jon Luck
2. Assessment of the red eye Visual acuity
Pain � nature, duration
Itchiness
Trauma?
Contact lens wear?
Discharge? � type � purulent? Mucous?
Past ophthalmic history � previous episodes?
3. Assessment of the red eye Lids � including eversion
Pupil reaction
Corneal clarity
Pre-auricular lymph nodes?
Stain with fluorescein
Magnification where possible
Fellow eye
4. Bacterial conjunctivitis We hardly ever see it!
Self-limiting
Neonates need referral (Chlamydia, Gonococcus)
Chloramphenicol, Fusidic acid
11. Scleritis Severe pain (cf episcleritis)
Associated with collagen vascular disease
Prompts investigation
Can be visually threatening
Requires systemic immunosuppression
12. Episcleritis Not painful (cf scleritis)
Not associated with systemic disease
Doesn�t prompt investigation
Never visually threatening
Doesn�t require systemic treatment
Associated Pinguecula
Topical NSAID�s (or weak topical steroids � under caution)
13. Iritis (Uveitis) Pain (esp on accommodation)
Photophobia
Recurrent
Systemic associations
Long term management
Patients experienced!
15. Angle-closure glaucoma Painful ++
Visual loss
Corneal oedema
Source of confusion in the elderly
Ophthalmic emergency
Requires systemic treatment
18. Microbial keratitis Bacteria cannot invade healthy cornea (exception Neisseria sp.)
Contact lens wearers
Dry eye
Previous surgery
Compromised ocular surface