Download
1 / 40
400 likes | 592 Views
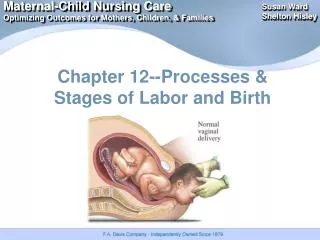
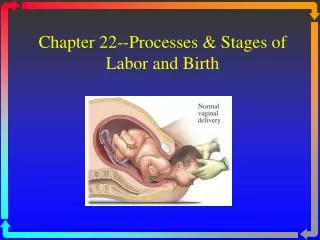
What is Labor ? (: work). Regular painful uterine contractions accompanied by progressive effacement and dilatation of the cervix. Timing of Labor. 40 weeks 8% deliver on E.D.C. 7% premature < 37 weeks 10% post-mature > 42 weeks.

E N D
What is Labor ?(: work) Regular painful uterine contractions accompanied by progressive effacement and dilatation of the cervix
Timing of Labor • 40 weeks • 8% deliver on E.D.C. • 7% premature < 37 weeks • 10% post-mature > 42 weeks
Signs of Onset of Labour “Show”Rupture of membranes Contractions
Detection of ruptured membranes Nitrazine Test - alkaline pH of fluidturns blue Ferning - high Na+ content causes“ferning” on air dried slide
Stages of Labor 1st stage - Onset to ‘full dilatation Latent active 2nd stage - Full dilatation to delivery of baby 3rd stage - Delivery of placenta 4th stage - Bonding
Table 30-1. Characteristics of Labor Nulliparas and Multiparas* Nulliparas Multiparas Characteristic All patients Ideal Labor All patients Ideal labor Duration of first stage (hr) Latent phase 6.4(±5.1) 6.1 (±4.0) 4.8 (±4.9) 4.5 (±4.2) Active phase 4.6(±3.6) 3.4(±1.5) 2.4(±2.2) 2.1 (±2.0) Total 11.0(±8.7) 9.5(±5.5) 7.2(±7.1) 6.6(±6.2) Maximum rate of descent (cm/hr) 3.3(±2.3) 3.6(±1.9) 6.6(±4.0) 7.0(±3.2) Duration of second stage (hr) 1.1(±0.8) 0.76(±0.5) 0.39(±0.3) 0.32(±0.3) * All values given are ± SD. (Data from Friedman EA: Labor: Clinical Evaluation and Management. 2nd ed. New York, Appleton-Century-Crofts, 1978).
Cesarean Section Indications Failure to progress Repeat (Failed VBAC) Fetal Distress Breech Presentation Placenta Previa Cord prolapse Abruption Diabetes Social...
DYSTOCIA DIAGNOSIS • Abnormal progression of labour in the ACTIVE Phase • Cervical dilatation of <0.5 cm/hr over a 4 hr period • arrest of progress in the ACTIVE phase either in the first or second stage of labour This includes a failure in the descent of the presenting part
OUTCOME OF PROLONGED LATENT PHASE • NCPP 1965 Apgar perinatal death and poor outcomewhere latent phase greater than 15 hours • Chelmow are 1993 - for labour intervention and low apgars where latent phase greater than 12 hours in nullip and 6 hours in multips • Piezner 1985 found that length of latent phase related to cervical dilatation on admission • Roemer 1996 found lower I.Q.’s in siblings with dystocia greater than 12 hours.
CAUSES OF DYSTOCIA Power Incoordinate uterine action Dysfunctional Labour Passenger CPD Relative disproportion Passages Diameters
DYSTOCIA • A 4 cm cut off separates latent from active labour • Abnormal progress never diagnosed before 4cm dilatation • Women not in active labour ‘triaged’ from the labour floor
CESAREAN SECTION FOR DYSTOCIA • Timing of procedure Rate • Latent phase 41% • Active phase 38% • Second stage 21% • Source: Stewart CMAJ 1990:142; 459-463
DYSFUNCTIONAL LABOUR - FACTORS OF INTEREST • Age • Parity • Infection • Epidural • Position in labour • Cervix • Induction • Macrosomia
INITIAL MEASURE TO TREAT DYSTOCIA • Comfort • wellbeing • hydration A. Attention to B. Amniotomy C. Oxytocin if A+B fail D. Wait long enough to see a response
OXYTOCIN USAGE Initial dose: 1 to 2 mlu/min Rate increased by 1 to 2 mlu/min every 30 min Until contractions are considered adequate and cervical dilatation achieved Clinical response usually seen at dose levels of 8 - 10 mlu/min
REDUCTION OF RISK OF DYSTOCIAFactors to avoid • Induction for large fetal weight • Oxytocin use with unfavourable cervix • No admission to Labour and Delivery at <4cm dilatation • Discontinuation of epidural at full dilatation • Immediate pushing after full dilatation
SUPPORTIVE STRATEGIES • Cervical evaluation for ripening prior to booking induction • Obstetrical triage • Continuous professional support in active labour • Mobilisation of women in active labour • Minimisation of motor blockage with epidural • Use of amniotomy and oxytocin prior to C/S for dystocia
APPROPRIATE MANAGEMENT FOR SLOW LABOUR ASSOCIATED WITH AN OCCIPITO POSTERIOR DURING THE FIRST STAGE OF LABOUR WOULD INCLUDE: a) immediate cesarean section b) forceps c) augmentation with oxytocin d) external cephalic version e) fetal blood sampling
NS NS -------------------------------------------- C C C C C C C