Download
1 / 3
30 likes | 126 Views
Name: Registration number: Address: Phone number: Office number: Mobile: Birth date: Sex: Marital status: Occupation: E-mail address: Referred by: Observations: Are you under medical treatment? Are you taking any medication? Which one?

E N D
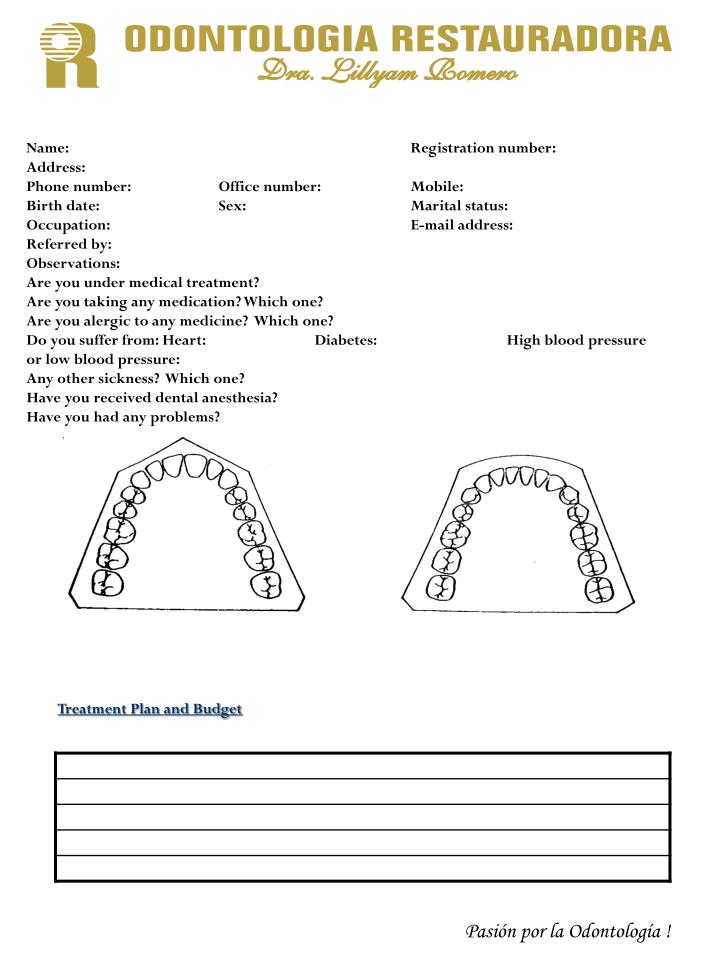
Name: Registration number: Address: Phone number: Office number: Mobile: Birth date: Sex: Marital status: Occupation: E-mail address: Referred by: Observations: Are you under medical treatment? Are you taking any medication? Which one? Are you alergic to any medicine? Which one? Do you suffer from: Heart: Diabetes: High blood pressure or low blood pressure: Any other sickness? Which one? Have you received dental anesthesia? Have you had any problems? Treatment Plan and Budget Pasión por la Odontología !
Before I finish this treatment I have to pay the total cost of it to Dra. Lillyam Romero. Name and signature: ______________________