Download
1 / 1
10 likes | 236 Views
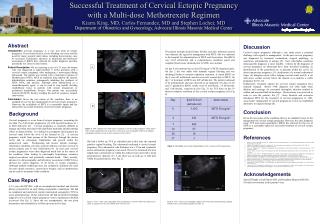
A Rare Case of a Cervical Ectopic Pregnancy. J WAHBA, N GARG, A KOTHARI Department of Obstetrics & Gynaecology, Hillingdon Hospital, London, United Kingdom. Introduction

E N D
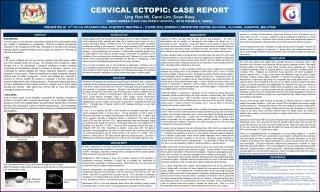
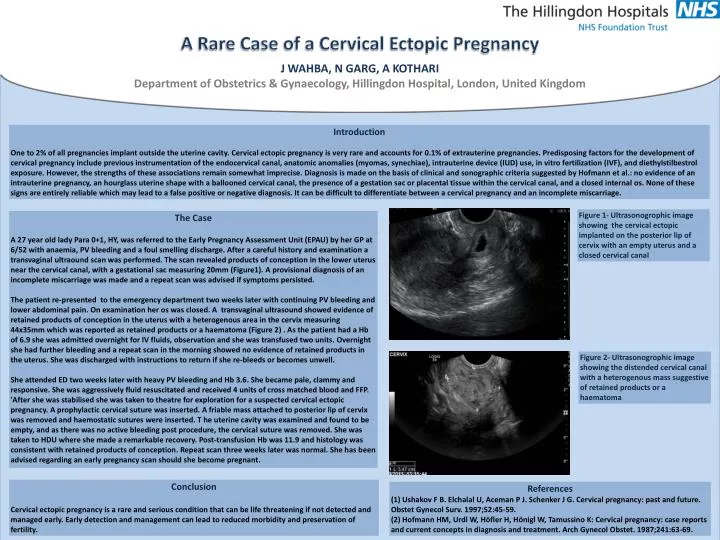
A Rare Case of a Cervical Ectopic Pregnancy J WAHBA, N GARG, A KOTHARI Department of Obstetrics & Gynaecology, Hillingdon Hospital, London, United Kingdom Introduction One to 2% of all pregnancies implant outside the uterine cavity. Cervical ectopic pregnancy is very rare and accounts for 0.1% of extrauterine pregnancies. Predisposing factors for the development of cervical pregnancy include previous instrumentation of the endocervical canal, anatomic anomalies (myomas, synechiae), intrauterine device (IUD) use, in vitro fertilization (IVF), and diethylstilbestrol exposure. However, the strengths of these associations remain somewhat imprecise. Diagnosis is made on the basis of clinical and sonographic criteria suggested by Hofmann et al.: no evidence of an intrauterine pregnancy, an hourglass uterine shape with a ballooned cervical canal, the presence of a gestation sac or placental tissue within the cervical canal, and a closed internal os. None of these signs are entirely reliable which may lead to a false positive or negative diagnosis. It can be difficult to differentiate between a cervical pregnancy and an incomplete miscarriage. Figure 1- Ultrasonogrophic image showing the cervical ectopic implanted on the posterior lip of cervix with an empty uterus and a closed cervical canal The Case A 27 year old lady Para 0+1, HY, was referred to the Early Pregnancy Assessment Unit (EPAU) by her GP at 6/52 with anaemia, PV bleeding and a foul smelling discharge. After a careful history and examination a transvaginalultraound scan was performed. The scan revealed products of conception in the lower uterus near the cervical canal, with a gestational sac measuring 20mm (Figure1). A provisional diagnosis of an incomplete miscarriage was made and a repeat scan was advised if symptoms persisted. The patient re-presented to the emergency department two weeks later with continuing PV bleeding and lower abdominal pain. On examination her os was closed. A transvaginal ultrasound showed evidence of retained products of conception in the uterus with a heterogenous area in the cervix measuring 44x35mm which was reported as retained products or a haematoma (Figure 2) . As the patient had a Hb of 6.9 she was admitted overnight for IV fluids, observation and she was transfused two units. Overnight she had further bleeding and a repeat scan in the morning showed no evidence of retained products in the uterus. She was discharged with instructions to return if she re-bleeds or becomes unwell. She attended ED two weeks later with heavy PV bleeding and Hb 3.6. She became pale, clammy and responsive. She was aggressively fluid resuscitated and received 4 units of cross matched blood and FFP. 'After she was stabilised she was taken to theatre for exploration for a suspected cervical ectopic pregnancy. A prophylactic cervical suture was inserted. A friable mass attached to posterior lip of cervix was removed and haemostatic sutures were inserted. T he uterine cavity was examined and found to be empty, and as there was no active bleeding post procedure, the cervical suture was removed. She was taken to HDU where she made a remarkable recovery. Post-transfusion Hb was 11.9 and histology was consistent with retained products of conception. Repeat scan three weeks later was normal. She has been advised regarding an early pregnancy scan should she become pregnant. Figure 2- Ultrasonogrophic image showing the distended cervical canal with a heterogenous mass suggestive of retained products or a haematoma Conclusion Cervical ectopic pregnancy is a rare and serious condition that can be life threatening if not detected and managed early. Early detection and management can lead to reduced morbidity and preservation of fertility. References (1) Ushakov F B. Elchalal U, Aceman P J. Schenker J G. Cervical pregnancy: past and future. ObstetGynecolSurv. 1997;52:45-59. (2) Hofmann HM, Urdl W, Höfler H, Hönigl W, Tamussino K: Cervical pregnancy: case reports and current concepts in diagnosis and treatment. Arch Gynecol Obstet. 1987;241:63-69.