Download
1 / 23
240 likes | 452 Views
Imaging the Pregnant Patient for Nonobstetric Conditions. What we are going to learn. What sequlae we are worried about Estimate of fetal radiation dose vs. modality. What might we do in some common scenarios. What’s the Big Deal?. Radiation-induced Teratogenesis

E N D
What we are going to learn • What sequlae we are worried about • Estimate of fetal radiation dose vs. modality. • What might we do in some common scenarios.
What’s the Big Deal? • Radiation-induced Teratogenesis • Radiation-induced Carcinogenesis • Increased risk for both leukemias and solid tumors
Estimated Fetal Dose • The natural background radiation dose to the fetus during pregnancy is approximately 1 mGy.
MR Imaging during Pregnancy • There has been no evidence of harmful effects at 1.5 T or lower. • Primary safety concerns: • Heating effects of radiofrequency pulses • Effects of acoustic noise on the fetus
Contrast Material • Iodinated Contrast: • Category B drugs; that is, animal reproduction studies have not demonstrated a fetal risk, • Gadolinium Contrast • Animal studies show growth retardation and congenital anomalies with doses 2-7x normal human dose
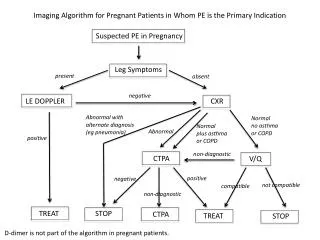
Imaging in Pulmonary Embolism • Pregnancy increases risk of venous thromboembolism by 5 • Radiation dose to the fetus from CT angiography of the maternal chest is similar to or lower than that from a ventilation perfusion scan • Consider modification of protocol
Imaging in Pulmonary Embolism Modifications That Decrease the Fetal Radiation Dose from Chest CT Angiography • Set the inferior limit of the scan just below the xiphoid process (to exclude the upper abdomen) • Increase the pitch and thicken the detector collimation • Eliminate the lateral scout view • Reduce the field of view and decrease the peak values for kilovolt peak and milliampereseconds (but not at the cost of image quality) • Do not scan the pelvis and lower extremities for possible deep vein thrombosis (ie, do not perform CT venography) • Use lead shielding (which is not an effective barrier for internal scatter but can decrease patient anxiety)
Imaging in Acute Appendicitis • Acute appendicitis is the most common nonobstetric emergency requiring surgery during pregnancy • Theoretical risk associated with an abdominal and pelvic CT study is approximately one cancer per 500 fetuses exposed to 30 mGy
Trauma and Pregnant Patient • Trauma is the leading nonobstetric cause of maternal death • Stabilize mother • Ultrasound fetus for Abruption/viability • Further diagnostic imaging as needed • Any examination that does not involve direct exposure to the maternal abdomen should be performed without concerns about fetal radiation effects
Counseling the PregnantPatient about Imaging Procedures • Decrease the anxiety • Use terms that can be understood by the patient • Risk of congenital anomalies, miscarriage, birth defects, or mental retardation is negligible • Risk of development of childhood cancer and leukemia is real, it is small • Imaging options available should be described, • Consequences of delaying or refusing imaging must also be explained
Bottom Line • The 1977 Report 54 of the National Council on Radiation Protection and Measurements contains the following statement: “The risk [of abnormality] is considered to be negligible at 5 rad (0.05 Gy) or less when compared to the other risks of pregnancy, and the riskof malformations is significantly increased above control levels only at doses above 15 rad (0.15 Gy). Therefore, the exposure of the fetus to radiation arising from diagnostic procedures would rarely be cause, by itself, for terminating a pregnancy.”
Summary • Diagnostic imaging is appropriate for diagnosing disease in pregnant women. • Diagnostic Imaging provides important information at sub-teratogenic levels • Diagnostic Imaging has a real but small risk of carcinogenesis. • Use appropriate modifications to minimize the fetal dose
Bibliography • Patel, SJ, Reede, DL, Katz DS, Subramaniam, R, Amorosa,JK. Imaging the Pregnant Patient for Nonobstetric Conditions: Algorithms and Radiation Dose Considerations. RadioGraphics 2007; 27:1705-1722