Download
1 / 13
140 likes | 522 Views
UOG Journal Club: November 2011. Ultrasound prediction of miscarriage. Accuracy of first-trimester ultrasound in the diagnosis of early embryonic demise: a systematic review Y. Jeve, R. Rana, A. Bhide, S. Thangaratinam

E N D
UOG Journal Club: November 2011 Ultrasound prediction of miscarriage Accuracy of first-trimester ultrasound in the diagnosis of early embryonic demise: a systematic reviewY. Jeve, R. Rana, A. Bhide, S. Thangaratinam Limitations of current definitions of miscarriage using mean gestational sac diameter and crown–rump length measurements: a multicenter observational study Y. Abdallah, A. Daemen, E. Kirk et al. Gestational sac and embryonic growth are not useful as criteria to define miscarriage: a multicenter observational study Y. Abdallah, A. Daemen, S. Guha et al. Clinical implications of intra- and interobserver reproducibility of transvaginal sonographic measurements of gestational sac and crown–rump length at 6–9 weeks gestation Pexsters, J. Luts, D. Van Schoubroeck et al. Volume 38, Issue 5, Date: November 2011, pages 489–515 (all articles) Journal Club slides prepared by Dr Tommaso Bignardi (UOG Editor for Trainees)
Diagnosis of miscarriage on TVS • American College of Radiologists (ACR) 2000 • CRL > 5mmwith no visible cardiac activity • MSD > 16mm without a visible embryo or yolk sac • Royal College of Obstetricians and Gynaecologists • (RCOG) 2006 • CRL ≥ 6mm with no visible cardiac activity • MSD ≥ 20mm without a visible embryo or yolk sac • Society of Obstetricians and Gynaecologists of Canada • (SOGC) 2005 • CRL > 5mm with no visible cardiac activity • MSD > 8mm without a visible yolk sac • MSD > 16mm without a visible embryo CRL, crown–rump length MSD, mean sac diameter
The current criteria used to diagnose miscarriage at ultrasound show variation Current guidelines are based on weak or moderate level of evidence (small studies or opinion) The accurate diagnosis of miscarriage is fundamental, as any error may be associated with inadvertent termination of a viable pregnancy
Accuracy of first-trimester ultrasound in the diagnosis of early embryonic demise: a systematic review Jeve Y et al., UOG 2011 Search of: • MEDLINE (1951 to 2011) • Embase (1980 to 2011) • Cochrane Library 720 citations reviewed, 23 met search criteria Eight articles involving a total of 872 women were included
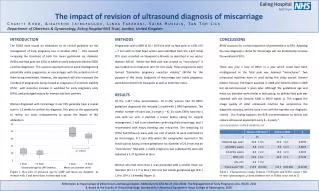
Results Best criteria have 95% CI range of 0.96 to 1.00 Jeve Y et al., UOG 2011 Nov
Conclusions Conclusions • First systematic review of ultrasound diagnosis of miscarriage • Studies are 15–20 years old, small numbers of miscarriage, reference standards were poor (method of miscarriage confirmation) • Various cut-off values used (4–6mm for CRL, 13–25mm for MSD), making pooling of data impossible • Best (most specific) criteria appeared to be MSD > 25mm with a missing embryo or MSD > 20mm with a missing yolk sac • These criteria had a 95% CI of 0.96–1.00, therefore up to 4 out of 100 diagnoses of early fetal demise may be wrong Jeve Y et al., UOG 2011 Nov
Limitations of current definitions of miscarriage using mean gestational sac diameter and crown–rump length measurements: a multicenter observational study Abdallah Y et al., UOG 2011 (a) Gestational sac and embryonic growth are not useful as criteria to define miscarriage: a multicenter observational study. Abdallah Y et al., UOG 2011 (b)
Multicenter observational study of 1060 women in four London hospitals Inclusioncriteria: - Intrauterine pregnancy of uncertain viability (IPUV) at sonography - IPUV defined as an MSD < 20mm with no obvious yolk sac/embryo orCRL < 6mm with no fetal heart activity Exclusioncriteria: - women clinically unstable - women who subsequently underwent uterine evacuation 2D-transvaginal scans (6–12 MHz) at 0 and 7–14 days later Abdallah Y et al., UOG 2011 (a)
Results: 1st scan cut-off values 1060 IPUV 473 (44.6%) viable at 11–13-week scan 587 (55.4%) non-viable at follow-up scans 1st scan Yolk sac - NO Embryo - NO MSD > 16mm FPR 4.4% MSD > 20mm FPR 0.5% MSD ≥ 21mm FPR 0% Yolk sac - YES Embryo - NO MSD > 16mm FPR 2.6% MSD > 20mm FPR 0.4% MSD ≥ 21mm FPR 0% Yolk sac - YES Embryo - YES CRL > 4mm FPR 8.3% CRL > 5mm FPR 8.3% CRL ≥ 5.3mm FPR 0% *FPR, false-positive rate for miscarriage at subsequent scans Abdallah Y et al., UOG 2011 (a)
Results: 2nd scan growth rate 1060 IPUV Subset of 359 patients where a gestational sac was seen on the second scan 7–14 days later 2nd scan Significant overlap of MSD and CRL growth between viable and non-viable pregnancies Failure to visualize a yolk sac or embryo on the follow-up scan was always associated with miscarriage Abdallah Y et al., UOG 2011 (b)
Clinical implications of intra- and interobserver reproducibility of transvaginal sonographic measurement of gestational sac and crown–rump length at 6–9 weeks' gestation Pexsters A et al., UOG 2011 Prospective cross-sectional study 54 women at 6–9 weeks • Observers blinded • CRL measured from the outer ends • Gestational sac measured in three planes • CRL and MSD measured twice by each observer
Results • Based on 95% CI, for a given CRL of 6mm as measured by one observer, the second observer’s measurement may range from 5.4 to 6.7mm • Similarly, given an MSD of 20mm as measured by one observer, the measurement for the second observer may range from 16.8 to 24.5mm Pexsters A et al., UOG 2011
Summary • Data from these studies show that current definitions used to diagnose miscarriage are potentially unsafe • Significant interobserver variability may be associated with a misdiagnosis of miscarriage • Current national guidelines should be reviewed to avoid inadvertent termination of wanted pregnancy • Large prospective studies with agreed reference standards are urgently required