Download
1 / 18
200 likes | 532 Views
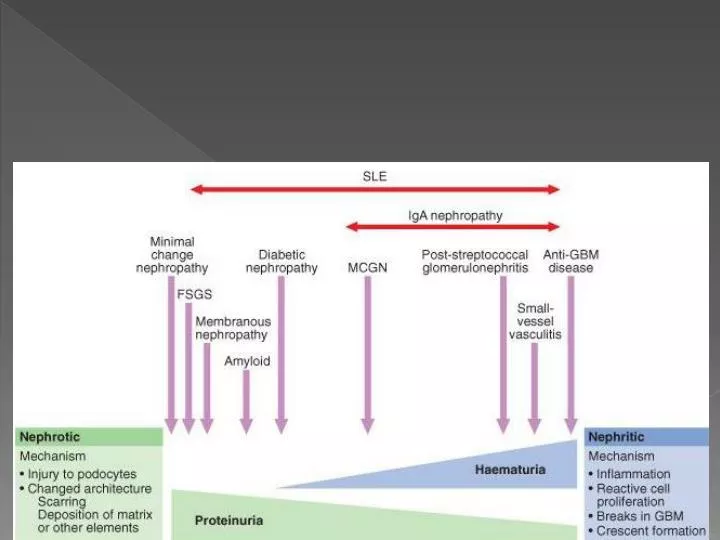
IgA nephropathy (Berger's disease) : Is named for the deposits of IgA in the glomerulus (Mesangium) Commonly seen in children & young adults It often affects young males within days (24-48hrs) after an upper respiratory tract or gastrointestinal infection.

E N D
IgA nephropathy (Berger's disease) : • Is named for the deposits of IgA in the glomerulus (Mesangium) • Commonly seen in children & young adults • It often affects young males within days (24-48hrs) after an upper respiratory tract or gastrointestinal infection. Microscopic examination • Shows increased number of mesangial cells with increased matrix Dr S Chakradhar
Presentation It usually presents as macroscopic haematuria (visibly bloody urine). • Gross hematuria often associated with URTI • Others present with asymptomatic hematuria accompanied by mild to moderate proteinuria. • Mild proteinuria of less than 1g/d is common, but the NS develops occasionally. Dr S Chakradhar
Serum IgA levels are increased in about 50% of cases but Serum complement is normal. • Immuno-staining is positive for immunoglobulin A deposits within the matrix. Treatment • Intermittent steroid therapy may reduce the frequency of episodes of gross of hematuria. • Steroids may also result in remissions of proteinuria in those patients with NS. Dr S Chakradhar
Prognosis • Is variable, but tends to progress slowly. • 50% of pts develop ESRF within 25 years of the time of diagnosis. • Poor prognostic indicators include proteinuria, hypertension, and azotemia. Dr S Chakradhar
Henoch-Schönlein purpura : • Is a systemic variant of IgA nephropathy which causes a small-vessel vasculitis and associated glomerulonephritis. • Deposition of immune complexes containing the antibody IgA in the skin and kidney Dr S Chakradhar
Membranoproliferative (MPGN)/ Mesangiocapillary GN : • There is thickening of GBM • Splitting of BM occurs due to inclusion of processes of mesangial cells • Proliferation of glomerular cells & mesangial cells Types • Primary - Idiopathic • Secondary to SLE, viral hepatitis Presents clinically as Nephrotic, Nephritic or mild proteinuria with inevitable progression to end stage renal failure Dr S Chakradhar
Minimal change GN : • No changes are visible on simple light microscopy, but on electron microscopy there is fusion of podocytes • This form of GN causes 80% of Nephrotic syndrome in children, but only 20% in adults. Dr S Chakradhar
Focal Segmental Glomerulo sclerosis (FSGS) : • Sclerosis of some but not all glomeruli • And only a segment of an individual glomerulus. May be • Primary (Idiopathic) • Secondary to reflux nephropathy, Alport syndrome, heroin abuse or HIV. • Presents as a Nephrotic syndrome • With varying degrees of impaired renal function (seen as a rising serum creatinine, hypertension). Dr S Chakradhar
Treatment • Steroids are often tried but not shown to be effective. • 50% of people with FSGS continue to have progressive deterioration of kidney function, ending in renal failure. Normal Dr S Chakradhar
Membranous glomerulonephritis : • Relatively common type of glomerulonephritis in adults, • Microscopically, MGN is characterized by a thickened glomerular basement membrane without a hypercellular glomerulus. • Immunofluorescence demonstrates diffuse granular uptake of IgG. Etiology • Idiopathic (85%) – taken as autoimmune disease • Secondary to systemic disease • Malignant epithelial tumors – ca of lungs & colon • SLE • Infections – chronic nephritis malaria syphillis, schistosomiasis • Drugs – captopril Dr S Chakradhar
Frequently produces a mixed nephrotic and nephritic picture. • Prognosis follows the rule of thirds: • 1/3rd remain with MGN indefinitely • 1/3rd remit and • 1/3rd progress to end-stage renal failure • The kidney appears to shrink. • Treatment with corticosteroids is attempted if the disease progresses. Dr S Chakradhar
RAPIDLY PROGRESSIVE (crescentic) GLOMERULONEPHRITIS (RPGN) • Crescents are formed in Bowman’s space by proliferating parietal epithelial cells with infiltrating monocytes & macrophage & sometimes neutrophils & lymphocytes • Reaches end stage renal failure within a period of days or weeks Dr S Chakradhar
Common Causes • Systemic vasculitis • SLE • Good Pasture’s (anti GMB) Disease • Aggressive phase of other inflammatory nephritis ( Ig A nephropathy, post infectious) Dr S Chakradhar
Patient presentation (Goodpasture’s syndrome) Adults, before the age of 30 years. A male predominance Onset generally preceded by upper respiratory infection • Renal failure develop rapidly, Severe oliguria • Symptoms like AGN – hematuria , proteinuria • Hypertension is uncommon • Pulmonary – haemoptysis & dyspnoe Diagnosis is confirmed by detecting anti – GBM antibodies Dr S Chakradhar
Treatment • Prednisolone plus cyclophosphamise or azathiprin • Plasma exchange to remove the Antiglomerular basement membrane antibodies in the plasma. Prognosis • Prognosis depends on the degree of irreversible glomerular damage. • Earlier diagnosis and treatment increases survival. Dr S Chakradhar
Chronic glomerulonephritis (CGN) • Is the final stage of GN when sclerosis has limited many glomeruli & their associated tubules • Persistent urinary abnormalities (proteinuria and/or hematuria) • Hypertension • Progressive loss of functioning Nephrons. • These patients generally progress to ESRD. Dr S Chakradhar
Treatment • Supportive and symptomatic. No specific treatment • Hypertension and infections should be treated vigorously. • Nephrotoxic agents should be avoided. Prognosis • Depends upon the nature of the underlying disease and presence or absence of complications, especially hypertension. • Ten, twenty, or more years may elapse from the first discovery of CGN until the development of ESRD. Dr S Chakradhar