Download
1 / 50
540 likes | 746 Views
2013 Joint meeting BNS-BSC. NOACs (new oral anticoagulants): are we ready for a wide use after stroke ? YES. George Ntaios University of Thessaly, Larissa, Greece. Leuven, Belgium. 23/11/2013. Disclosures.

E N D
2013 Joint meeting BNS-BSC NOACs (new oral anticoagulants): are we ready for a wide use after stroke?YES George Ntaios University of Thessaly, Larissa, Greece Leuven, Belgium 23/11/2013
Disclosures • Support to attend conferences: Bayer; Sanofi-Aventis; Pfizer; Lundbeck; Boehringer-Ingelheim;Galenica;Elpen; Bristol Myers Squibb. • Honoraria: Quintiles; CHUV; Medtronic. • Speaker fees: Sanofi • Scholarships: European Stroke Organization; Hellenic Society of Atherosclerosis. • Participation in trials • National coordinator (Greece) for the ENOS trial. • Sub-investigator (AMGEN, 20110118).
Intracranialhemorrhage Ischemic stroke 20 • Target INR 2.5 • (range 2-3) 15 Odds ratio 10 5 1.0 2.0 3.0 4.0 5.0 6.0 7.0 INR Courtesy of Patrik Michel, adapted from Hylek et al. NEJM 1996; 335:540-6
Why is it so difficult ? Inactive precursor Active Clotting Factor - Diet Oxidised Vitamin K Reduced Vitamin K Vitamin K oxide reductase CYP1A1 CYP1A2 CYP3A4 CYP2C9 S R WARFARIN
Inactive precursor Active Clotting Factor - Diet - Drugs Oxidised Vitamin K Reduced Vitamin K Vitamin K oxide reductase CYP1A1 CYP1A2 CYP3A4 CYP2C9 S R WARFARIN
Corticotropin Cortisone Coumadin Cyclophosphamide Danazol Dextran Dextrothyroxine Diazoxide Diclofenac Dicloxaxillin Diflunsial Disulfram Doxycycline Erythromycin Ethacrynic acid Ethchlorvynol Fenoprofen Fluconazole Fluorouracil Gemfibrozil Glucagon Glutethimide Griseofulvin Haloperidol Halothane Heparin Ibuprofen Ifosamide Indomethacin Influenza virus vaccine Itraconazole Ketoprofen Ketorolac Levamisol Levothyroxine Liothyronine Lovastatin Mefenamic Meprobamate Methimazole Methyldopa Methylphenidate Methylsalicylate Miconzale Metronidazole Miconazole MoricizineHCl Nafcillin Nalidixic acid Naproxen Neomycin Norfloxacin Ofloxacin Olsalazine Omeprazole Oxaprozin Oxymetholone Paraldehyde Paroxetine Penicillin G Pentobarbital Pentoxifylline Phenobarbital Phenylbutazone Phenytoin Piperacillin Piroxicam Prednisone Primidone Propafenone Propoxyphene Propranolol Propylthiouracil Phytonadione Quinidine Quinine Ranitidine Rifampin Secobarbital Sertaline Simvastatin Spironolactone Stanozolol Streptokinase Sucralfate Sulfamethizole Sulfamethoxazole Sulfinpyrazone Sulfinpyrazone Sulfisoxazole Sulindac Tamoxifen Tetracycline Thyroid hormone Ticacillin Ticlopidine t-PA Tolbutamide Trazodone Trimethoprim-sulfamethoxazole Urokinase Valproate Vitamin C Vitamin E Abciximab Acetaminophen Alcohol(acute and chronic) Allopurinol Aminodarone Aminoglutethimide Amobarbital Anabolic steroids Aspirin Azathioprine Butabarbital Butalbital Carbamazepine Cefoperazone Cefotetan Cefoxitin Ceftriaxone Chenodiol Chloral hydrate Chloramphenicol Chlorpropamide Chlorthalidone Cholestyramine Cimetidine Ciprofloxacin Clarithromycin Clofibrate
Inactive precursor Active Clotting Factor - Diet - Drugs - Polymorphisms Oxidised Vitamin K Reduced Vitamin K Vitamin K oxide reductase CYP1A1 CYP1A2 CYP3A4 CYP2C9 S R WARFARIN
Age(years)CYP2C9*1CYP2C9*2CYP2C9*3 6.5 (2.9, 10.2) 6.3 (2.7, 9.9) 6.0 (2.5, 9.6) 5.8 (2.2, 9.3) 5.5 (2.0, 9.0) 5.3 (1.8, 8.8) 5.0 (16, 8.5) 4.8 (1.3, 8.2) 4.5 (1.1, 7.9) 4.3 (0.9, 7.7) 4.0 (0.6, 7.4) 3.8 (0.4, 7.2) 3.5 (0.9, 6.9) 3.3 (-0.2, 6.7) 3.0 (-0.5, 6.5) 5.8 (1.9, 9.8) 5.6 (1.8, 9.4) 5.3 (1.6, 9.0) 5.1 (1.5, 8.7) 4.8 (1.3, 8.3) 4.6 (1.1, 8.0) 4.3 (1.0, 7.7) 4.1 (0.8, 7.4) 3.8 (0.5, 7.1) 3.5 (0.3, 6.8) 3.3 (0.1, 6.5) 3.0 (-0.2, 6.3) 2.8 (-0.5, 6.0) 2.5 (-0.8, 5.8) 2.3 (-1.1, 5.6) 5.5 (1.3, 9.8) 5.3 (1.2, 9.4) 5.0 (1.1, 9.0) 4.8 (1.0, 8.6) 4.5 (0.8, 8.3) 4.3 (0.7, 7.9) 4.0 (0.5, 7.5) 3.8 (0.3, 7.2) 3.5 (0.1, 6.9) 3.3 (-0.1, 6.6) 3.0 (-0.3, 6.4) 2.8 (-0.6, 6.1) 2.5 (-0.8, 5.9) 2.3 (-1.1, 5.7) 2.0 (-1.5, 5.5) Estimated warfarin daily dose (mg) based on patient age and genotype 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 Thrombosis & Anticoagulation Research Group
“… lower initiation doses should be considered for patients with certain genetic variations in CYP2C9 and VKORC1 enzymes …” FDA 2007
45.2% 45.4% Kimmel, et al. NEJM 2013, online early
61.6% 60.2% Verhoef, et al. NEJM 2013, online early
67.4% 60.3% Pirmohamed, et al. NEJM 2013, online early
Anti-VKAs’ limitations Narrow therapeutic window Frequent INR monitoring Frequent dose adjustments Unpredictable dose response Drug and food interactions Slow onset/offset of action
Anti-VKAs’ limitations Narrow therapeutic window Frequent INR monitoring Frequent dose adjustments Unpredictable dose response Drug and food interactions Slow onset/offset of action
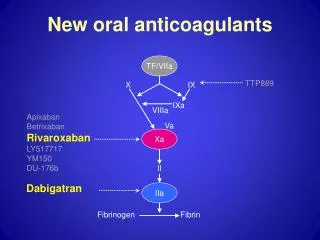
Rivaroxaban Apixaban Edoxaban Dabigatran Acenocoumarol Warfarin
NOAC’s limitations (?) • Patients with renal function impairment • Patients with mechanical valves • Can not monitor drug effect and titrate dose • No specific antidote • Their short half-life makes them dangerous in non-adherent patients • Not better than warfarin for high TTRs Eerenberg, et al. Circulation 2011; 124:1573-9 Majeed, et al. Circulation 2013; 128:2325-32
NOAC’s limitations (?) • Patients with renal function impairment • Patients with mechanical valves • Can not monitor drug effect and titrate dose • No specific antidote • Their short half-life makes them dangerous in non-adherent patients • Not better than warfarin for high TTRs • Bleeding rates in real-life were higher than in RCTs
“We believe that the large number of reported cases of bleeding associated with dabigatranprovides a salient example of stimulated reporting.” “Bleeding rates associated with dabigatran are not higher than those with warfarin, a finding that is consistent with the results of RE-LY.” “We believe that dabigatran provides an important health benefit when used as directed.” Southworth M, et al. NEJM 2013; 368:1272-4
NOAC’s limitations vs. Warfarin • Reduce stroke or systemic embolism • Reduce ICH • Reduce major hemorrhage • Steady dose • Limited drug & no food interactions • No INR monitoring Novel oral anti-coagulants
NOACs (new oral anticoagulants): are we ready for a wide use after stroke? YES THIS IS ALREADY HAPPENING !
Kirley K, et al. Circ Cardiovasc Qual Outcomes. 2012;5:615-621