Download
1 / 20
200 likes | 356 Views
ten years follow up of hereditary hemorrhagic patients in the dental practice. Makris SP, Makris MP, Makris PE Haemostasis and Thrombosis Unit, Aristotle University of Thessaloniki, Greece. introduction. the provision of dental care in hereditary hemorrhagic patients was always a challenge

E N D
ten years follow up of hereditary hemorrhagic patients in the dental practice Makris SP, Makris MP, Makris PE Haemostasis and Thrombosis Unit, Aristotle University of Thessaloniki, Greece
introduction the provision of dental care in hereditary hemorrhagic patients was always a challenge pain + bleeding kept away patients from the dentist
introduction I • the last 10 years we are trying to make dental procedures more comfortable and less complicated to this group of patient • in order to accomplice that, we thought that preventionmust be the key word
introduction II • regular periodic preventive checkout • examination – teeth cleaning – instructions • early care of dental problems • fillings, endodontic treatments, teeth scalings to avoid teeth loss
introduction III • bloodless confrontation of the mainly hemorrhagic interventions • tooth extraction, cyst excision, apicoectomy • proper measures during the apoptosis of deciduous teeth
material Ι • 160 adults hemophiliacs A+B (155+5) • 255 adults with vWD • 25 childrenmostly hemophiliacs
work protocol I • with the criterion of DDAVP response we divided our group of patients in II categories • responders • coverage with ddavp during dental procedure when needed • non-responders • coverage with 40 units/kg-BW of recombinate factorsduring dental procedure when needed
work protocol II √ splint • to both groups local haemostasis measures were the same √ fibrin sealant √ suture √ surgicel √ collagen fleece √ pressing tampon √ tranexamic acid
our experience I while we started with the use of splint in all patients, we observed: • the splint in young patients had to be replaced every now and then and hence discomfort and extra cost. (because of their growing) • the placement of splint in adults was not always possible (because of the morphology of teeth). • they exists more procedures where the splint cannot offer local haemostasis (extraction of impacted tooth, apicoectomy , cyst excision)
our experience II • we replaced the splint with fibrin sealants with very good results, but also with considerably increased cost of work
our experience III • we observed that the gauze surgicel although it was extremely effective, it easily induced superficial infections, what however they could jeopardise the fragile balance of wound at the first post-operative hours.
our experience IV • because of that we replaced it with collagen fleece in combination with pressing tampon with very good results so far.
our experience V • suturing in combination with surgicel or collagen fleece and pressing tampon in all cases of minor oral surgery
our experience VI • 10% aqua solution of tranexamic acid (for 10 days) as a mouth rinse had been used all those years with no exception in any dental procedure where blood could be involved (from a teeth cleaning to a teeth extraction).
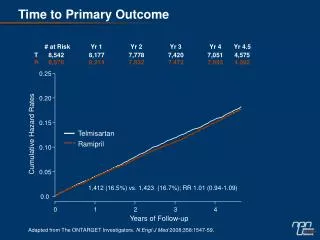
results 1=NO bleeding 2=RARE bleeding 3= FREQUENT bleeding 4=REPEATED bleeding
today’s standard protocol responders
today’s standard protocol non-responders
conclusion with our occupation with the oral cavity of patients with hereditary haemorrhagic diathesis, we conclude the following: • dental action was rendered blood-free • this installed the foundation of confidence in the dentist’s face • it removed the hesitations and the phobias of the past • ensured the acceptance of preventive dental measures.