Download
1 / 89
900 likes | 1.16k Views
It’s Leaky. MITRAL REGURGITATION Rami Khouzam, MD. Mitral Regurgitation. Anatomy: 3 basic mechanisms of MR: 1- Alteration of Mitral leaflets, commissures, or annulus 2- Defective tensor apparatus 3- Alterations of LV and LA size & function.

E N D
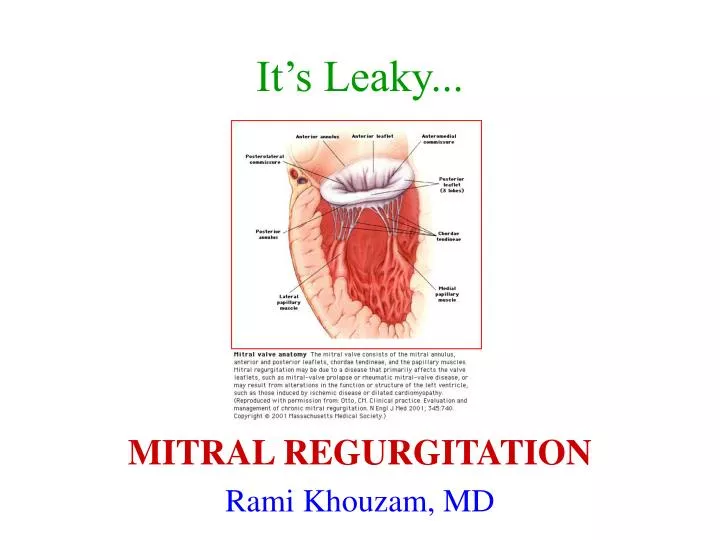
It’s Leaky... MITRAL REGURGITATION Rami Khouzam, MD
Mitral Regurgitation • Anatomy:3 basic mechanisms of MR: • 1- Alteration of Mitral leaflets, commissures, or annulus • 2- Defective tensor apparatus • 3- Alterations of LV and LA size & function
1- Alteration of Mitral leaflets, commissures, or annulus: • MVP: most common cause of isolated MR. Posterior leaflet more frequent and severe. Greater in men. Increases with age. • Rheumatic fever • Mitral annulus calcification: age-related • Infective endocarditis • Congenital: cleft of anterior MV associated with primum ASD
2- Defective tensor apparatus: • Abnormal chordae tendineae: Idiopathic/ endocarditis/ MVP/ Trauma • Papillary muscle dysfunction: • Posteromedial > anterolateral (vulnerability to ischemia & infarction): single blood supply
3- Alterations of LV and LA size & function: • Alteration of position and axis of papillary muscle • Mitral ring dilatation
Key points... • Mitral prolapse is the most common cause of isolated MR • Ischemia: dysfunction/rupture of papillary muscle. Posteromedial > anterolateral • LV enlargement & abnormal contractile function are common causes of MR
Pathophysiology of MR • 1. Acute Stage • 2. Chronic Compensated Stage • 3. Chronic Decompensated Stage
Key points... • Acute severe MR is characterized by normal-sized chambers, high EF, & pulmonary congestion. • Chronic compensated severe MR is typified by few symptoms, enlargement of the LV & LA, and high EF • Chronic decompensated severe MR is typified by enlargement of the LV & LA, pulmonary congestion, and normal to low EF • A “normal range” EF in the setting of severe MR usually implies LV systolic dysfunction
Clinical syndrome of MR • Acute MR • If severe: pulmonary congestion • S3 S4 • Systolic murmur: short, soft or absent
Chronic MR • Prolonged asymptomatic interval. • Fatigue/ generalized weakness • Laterally displaced, enlarged apical impulse • Severe MR: apical thrill • Early aortic closure • Holosystolic murmur: intensity does not correlate with severity of regurgitant flow • Anterior leaflet MR: Radiates to axilla frequently • Posterior leaflet abnormality: regurgitant flow anteriorly radiation to aortic area, and all precordium • Short diastolic apical rumble in the absence of MS: high diastolic transmitral flow & severe MR
Key points... • Acute severe MR: short or soft murmur because of low LV-LA pressure gradient • Nonspecific fatigue & weakness may represent early symptoms of chronic severe MR • Duration of apical impulse in chronic severe MR is related to LV systolic function • Posterior leaflet prolapse: murmur to aortic area • Amyl nitrite distinguishes diastolic rumble of mixed MS & MR () from that due to isolated severe MR ()
Evaluation of MR • EKG • LAE • Atrial fibrillation • LVH • Nonspecific ST-T changes • CXR • LVE • LAE (straightening left border, atrial double density, elevation of left main-stem bronchus) • Pulmonary venous congestion
Echocardiography • In some cases, TEE is better to assess the anatomy of the MV, to rule out atrial thrombus, gather supplemental data in quantitative & qualitative measures of regurgitation severity (but not always necessary).
Determination of severity • Over 20 variables described. • Color flow Doppler • Atrial side: • Small jet occupying < 20 % of LA: mild • 20- 40 %: moderate • Large jet > 40 % and extending into the pulmonary veins): severe • Ventricular side: PISA proximal flow acceleration (proximal isovelocity surface area): concentric series of hemispheric rings of alternating colors, each ring denoting an isovelocity of aliasing. The diameter of the ring closest to the regurgitant orifice is measured and, in severe mitral regurgitation, usually approaches • 1 cm.
Pulsed and continuous wave Doppler of mitral inflow • E > 1.4 m/sec • E/A ratio > 2 • (Finding an A-wave dominant pattern of mitral inflow makes severe mitral regurgitation very unlikely). • Uniformly dense jet throughout its duration, well-defined envelope • TR peak velocity: pulmonary hypertension. • Doppler of pulmonary veins: show systolic flow reversal
Doppler of pulmonary veins • (pulse Doppler of the left and right upper pulmonary veins from the apical four-chamber view). Normal pulmonary venous flow is antegrade during both ventricular systole and diastole (ventricular systolic component dominates), with slight retrograde flow during atrial systole. In hemodynamically severe mitral regurgitation, the flow in one or more pulmonary veins (depending upon the direction of the jet) will show systolic flow reversal
Index of severity • Based on 6 variables, each scored on a scale of 0 to 3 then averaged • 1- Color Doppler regurgitant jet width and penetration2- Color Doppler PISA diameter3- Continuous wave Doppler characteristics of the regurgitant jet4- Continuous wave Doppler TR derived PAP • 5- Pulse wave Doppler pulmonary venous flow pattern6- Left atrial size by 2D- echocardiography • (Mild MR: index 1.7, Severe MR (regurgitant fraction >40 percent) : index 1.8, A value 2.2 identified patients with severe mitral regurgitation with a sensitivity, specificity, and positive predictive value of 90, 88, and 79 percent, respectively).
Cardiac catheterization • Right heart cath: Prominent “V” wave on PCWP tracing • Left heart cath/ Ventriculogram: Only when - noninvasive data are discordant or • - technically limited or • - differ from the clinical perception of the severity of MR or ventricular function. • Angiographic grading: many variables..
Key points... • No EKG or CXR findings pathognomonic of MR • Echo is invaluable for assessing cause & severity of MR, size and function of LV, LA, RV • Left ventriculography is most useful when noninvasive data discordant or technically limited or differ from clinical impression of the severity of MR, or ventricular function
Mitral valve prolapse • Click: systolic billowing of a portion of mitral leaflet into LA • Maneuvers that ventricular preload (Valsalva, standing): prolapse, click & murmur earlier in cardiac cycle. • Progression to severe MR: more in men, and advancing age • MVP & severe MR: managed as severe MR • Antibiotic prophylaxis: when? • - Click & murmur, or • - Click & echo: significant leaflet thickening or regurgitation • B-Blocker: for MVP/palpitations/atypical CP/anxiety • ASA: TIA in the setting of MVP
Natural history of MR • Depends on its cause • Time course of progressive LV dysfunction in chronic MR is variable & unpredictable • Acute worsening of MR suggests chordal rupture, infection, new arrhythmia, or ischemia
Outcome after surgical correction of MR (The unnatural history) • Current surgical practice is to operate on patients with severe MR before the development of heart failure or ventricular dysfunction, if possible • Preoperative EF: best predictor of long-term mortality, CHF, & postoperative LV function • End-systolic dimension: significant predictor • A. fib more than 3 months preoperatively associated with high risk of postoperative arrhythmia persistence and need for long-term anticoagulation
Treatment of Acute severe MR • i.v. vasodilators (Na nitroprusside), • i.v. inotropes, IABP • Mitral valve Repair or Replacement • Endocarditis: delay surgery if possible (risk of recurrence), unless progressive heart failure, unresponsive to antibiotics, intracardiac abscess, recurrent systemic embolization
Treatment of Chronic Nonischemic MR • Dental hygiene/ Antibiotic prophylaxis • Treat contributing underlying disease • No data to indicate diuretics or vasodilators (or both) provide morbidity or mortality benefit • Every patient should be considered for surgery
MV REPAIR • Who gets it?? • Repair should be performed preferentially whenever possible: favorable predictor of operative mortality, late survival, postoperative EF. • High risk patients: severe LV dysfunction (EF < 35 %, • CI < 1.5 L/min per m2) • MR: posterior leaflet, non-rheumatic, noninfective, noncalcific, nonischemic: most amenable to repair
Treatment of MR d.t. Ischemia or Cardiomyopathy • Maximal medical therapy: FIRST • MVR (Mitral annular rings)
Key points... • Patients with acute severe MR & hemodynamic instability require rapid evaluation, aggressive stabilization, & early valve operation • Patients with acute severe MR & hemodynamic stability: semielective surgery • Indications for valve surgery in endocarditis: progressive heart failure, resistance to antibiotics, intracardiac abscess, recurrent systemic embolization despite therapy • Severe chronic MR & NYHA class III or IV, EF < 60 %, End-systolic diameter > 45 mm, or end-systolic volume > 50 mL/m2: Definite Surgery
Key points... • Emerging indications for MV Replacement: Flail leaflet, paroxysmal or recent A. Fib, pulmonary HTN • Impaired LV function: Valve repair preferred • NO Repair in: • rheumatic, ischemic, endocarditis, anterior or bileaflet prolapse, significant calcification