Download
1 / 41
410 likes | 601 Views
Fetal circulatio n. Dr. S. Parthasarathy MD., DA., DNB, MD ( Acu ), Dip. Diab.DCA , Dip. Software statistics PhD ( physio ) Mahatma gandhi medical college and research institute, puducherry , India. What are the needs of the CVS ??. Give oxygen to tissues

E N D
Fetal circulation Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab.DCA, Dip. Software statistics PhD (physio) Mahatma gandhi medical college and research institute, puducherry, India
What are the needs of the CVS ?? • Give oxygen to tissues • Give metabolic nutrients to tissues
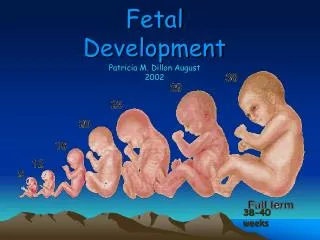
Essence • The entire cardiac output cannot go to the lungs • Hence we have shunts in the circulation • But adequate oxygen supply has also be there • After delivery, lungs take over, shunts disappear • The foramen ovale, ductusarteriosus, and ductusvenosus
Some changes take place • That is transitional circulation • Word is important – transitional !!! • If it is permanent – think of preterm, critically ill neonate or congenital cardiac illness
Special characters • Parallel arrangement of two main arterial systems and their respective ventricles. • But series in adults • Mixing of venous return and preferential streaming. • High resistance, low flow of pulmonary circulation. • Low resistance and high flow of placental circulation. • Presence of shunts
The pathway • Deoxygenated blood of fetus • Descending aorta • Umbilical arteries Placenta • Intervillous spaces - gas exchange oxygenated blood
Then what happens • Umbilical vein • Preferably through ductusvenosusto IVC • Streaming • Liver bypassed
From the IVC, it bypasses the right atrium through foramen ovaleto Left atrium
Streaming • Eustechian valve helps to direct the IVC blood to cross the foramen ovale to left atrium • The lower margin of septum secundum [cristadividens] helps to direct the left posterior stream to preferentially across the foramen ovale. • Posterior and left stream of IVC blood carries oxygenated blood while anterior and right stream carries poorly oxygenated blood • SVC blood is directed across the TV to right ventricle
Left atrium to left ventricle through mitral valve • LV to ascending aorta • Supplies oxygenated blood to three main arteries • Mixes with ductusarteriosus blood
most highly oxygenated blood is delivered to the myocardium and brain.
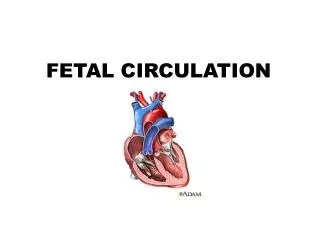
The pathway • Deoxygenated blood from the SVC and part of IVC enter Right atrium, • Tricuspid valve • Right ventricle • Pulmonary artery • Then lungs ?? No • But through ductusarteriosus to descending aorta
Left to right (blue) • And • Right to left shunt (Pink) • follows
60 50 65 80 % 25%
RV vs LV • The RV receives about 65% of the venous return and the LV about 35%. • Thus, in the shunt dependent circulation of the fetus, the situation is much more complex and cardiac output must be defined in different terms. • Hence CVO = combined ventricular output • 45 % to placenta 8 % to lungs
The big three • high hemoglobin (16gm%) • fetal haemoglobin • high CVO • help maintain oxygen delivery in the fetus despite low oxygen partial pressures
HbF Normal Hb
Transition • Gas exchange function is transferred from placenta to the lungs. • Shunts closure • Separation of systemic and pulmonary circulations. • LV output must increase • Increased metabolism to maintain body temperature
What is done • Placenta removed • Cord clamped • Baby cries and lung starts to inspire
Cord clamped and placenta removed • The umbilical vessels are reactive and constrict in response to longitudinal stretch and the increase in blood PO2. • Obviously external clamping of the cord will augment this process. • Placenta removed • No flow through ductusvenosus
Lungs expand • At birth, after expansion of the lungs, there is a dramatic fall in PVR and an 8–10-fold increase in pulmonary blood flow. • Expansion stimulation of stretch receptors vasodilation • Not oxygen , even any gas
Initial closure of the foramen ovale occurs within minutes to hours of birth. • Anatomical closure occurs later via tissue proliferation. • Ductusvenosus is closed FO closed , what next • Ductusarteriosus
Concomitant with the drop in PVR, the shunt at the level of the DA becomes bi-directional. • The exact mechanism of ductal closure is not known • increased PO2 in neonatal blood- direct constriction of smooth muscle within the duct. • concentrations of PGE2, produced in the placenta, fall rapidly after birth, causes ductal constriction.
Ductusarteriosus • Functional closure by 96 hours • anatomical closure via endothelial and fibrous tissue proliferation later • Hemoglobin • HbF becomes adult Hb – better oxygen delivery
Cardiac output • Term fetus -- CVO = 400 ml / kg/min. • Neonate CVO = upto 400 ml / kg/min. • Upto 4.0 litres / sq. metre • Necessary for increased metabolic demands • LV and RV outputs equalize
By then-- why we should know about fetal circulation • Take for example – A case of truncus or transposition of vessels come for other surgery – It should be known to us that Ductusarteriosus should be kept patent – • Yes they need shunts • We can start PGE1 infusions • Congenital diaphragmatic hernia – PVR has not come down – What should be done to make fit !!