Download
1 / 11
260 likes | 1.53k Views
Anatomical aspect of the fetal circulation Role of the shunts and their regulation Ductus arteriosus Foramen ovale Ductus veinosus Fetal cardiac output / particularities of the fetal heart Modification at birth of the fetal circulation. Fetal Circulation. Fallot’ Project.

E N D
Anatomical aspect of the fetal circulation Role of the shunts and theirregulation Ductusarteriosus Foramen ovale Ductusveinosus Fetalcardiac output / particularities of the fetalheart Modification atbirth of the fetal circulation Fetal Circulation Fallot’ Project 2sdDecember 2009
References • Rudolph AM. Circ. Res. 1985; 57; 811-821 • Kiserud T and Rasmussen S. UltrasoundObstetGynecol 2001; 17: 119–124 • Jouannic J.-M , Fermont L, Brodaty G, Bonnet D, Daffos F. J GynecolObstetBiolReprod 2004 ; 33 : 291-296.
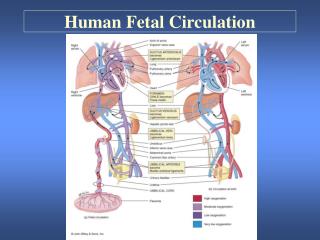
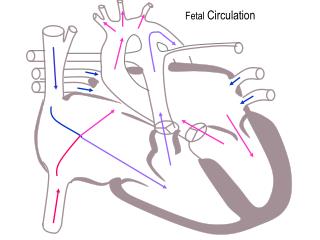
FetalCirculation Ductusarteriosus lungs Foramen ovale liver aorta Anatomic aspect Ductusveinosus (Arantius canal) Umbilicalvein placenta Placenta serves as the site for gasexchange Umbilicalarteries Umbilicalcord
Role of the shunts Orientateoxygenatedblood flow to the supra-aortic parts (brain / heart) UmbilicalVein -> DV -> IVC -> RA -> FO -> LA -> LV -> ascendingaorta Orientatedeoxygenatedblood flow to the infra-aortic partstoward the placenta IVC -> RA -> RV -> PA -> DA -> descendingaorta
Role of the foramen ovale Preferential flow from the IVC and from the right hepaticvein(anterior part of the IVC) to the right ventricle (less or deoxygenatedblood flow) Preferential flow from the ductusveinosus (U.V.) and from the lefthepaticvein(posterior part of the IVC) to the foramen ovale then to the leftventricle(oxygenatedblood flow) Orientateoxygenatedblood flow to the supra-aortic parts (brain / heart) Hypothesis : the streamlining of flows in the inferior vena cava « Anatomical canal » into the RA (Eustachian valve) helps direct the flow into the LA via FO Difference of the velocitiesbetween the twoflows. Kiserud T. Fetalvenous circulation — an update on hemodynamics. J Perinat Med 2000; 28: 90-6.
Role of the ductusarteriosus High pulmonaryvascularresistances Shunt from RV and PA to the descendingaorta Regulation: Vasodilatation Prostaglandin (PGE) Low PO2 Vasoconstriction Indomethacin Endothelin 1 (<= smoothmuscularcells / endothelium) High PO2 (atbirth)
Role of the ductusveinosus 50% of the blood flow comingfrom the umbilicalveinbypasses the liverand goesdirectly to the leftventriclethrough the foramen ovale (70% in case of hypoxemia or hypovolemia) The O2 extraction by the liverisweak: only 15% Importance of the flow’sregulation in case of decreasing of the pressure into the umbilicalvein: prostagladins, CO, adrenergic system,… i.e.: whenumbilicalvenousreturn is progressively reduced the percentage of umbilical venous blood passing through the ductusvenosusincreasesprogressively 40% 5%
Fetalcardiac output (425ml/mn/kg) • The factors that influence cardiac output are heart rate, filling pressure or preload, compliance of the ventricles, resistance against which the ventricles eject, or afterload, and myocardial contractility. • Fetalmyocardialcompliance • Lowerpossibility to increase the stroke volume afterincreasing of the preloadthan in an adultheart(lesscompliant) • Fetalmyocardialcontractility • Difficulty to support stroke volume afterincreasing of the postload
Percentages of combinedventricular output ejectedby eachventricle from Rudolph / CircRes 1985 20% SVC 10% 70% IVC
Modification of the fetal circulation Pulmonary output => Only 10% of the combinedoutput Atbirth : Importante decreasing of the pulmonaryresistances: Mechanicalfactors Vasoactive substances: NO / PO2 Increasing of: pulmonaryoutflow leftvenous return => closure of the foramen ovale(Vieussens valve) High PO2 => vasoconstriction of the D.A.
Oxygen saturations 50% 65% 35% 70%