Download
1 / 26
260 likes | 762 Views
The Demise of AWP or We are all WAC'd Changes to Pharmacy Reference Pricing . Learning Objectives. Identify current Average Wholesale Price (AWP) publishing stateIdentify AWP benchmark alternatives for adjudicationDetermine transparency of pricing benchmarksUnderstand pharmacy acquisition costs vs. pricing benchmarksReview market response to pricing benchmark instability.

E N D
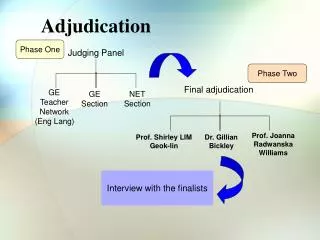
1. Pharmacy Adjudication Alternatives to AWP Pharmacy Benefits Academy
August 19, 2010
Alan L. Van Amber
Vice President, Pharmacy Network Management
Navitus Health Solutions
3. Learning Objectives Identify current Average Wholesale Price (AWP) publishing state
Identify AWP benchmark alternatives for adjudication
Determine transparency of pricing benchmarks
Understand pharmacy acquisition costs vs. pricing benchmarks
Review market response to pricing benchmark instability
4. What is AWP? Average Wholesale Price (AWP)
Does not actually mean the average wholesale price!
Despite its name, AWP is not an average of prices charged by wholesalers to providers
AWP is not transparent in its determination
Brands: AWP is often a mark-up by drug compendia of wholesale acquisition cost (WAC)
Generics: AWP is often a manufacturer list price with no real calculation schema
AWP is widely published For BRAND products
Based upon the Wholesale Acquisition Cost (WAC), which is the price that wholesalers pay to purchase the drug from the manufacturer. The WAC is marked-up by a fixed factor � typically 1.20 or 1.25 � to generate the AWP. Neither the determination of WAC nor the determination of AWP is subject to regulatory review.
Pharmaceutical companies make a prescription drug and assign it a price for sale in the
pharmacy distribution system, mostly through pharmaceutical wholesalers. The price is
referenced as Wholesale Acquisition Cost (WAC).
Step 2
Pharmaceutical wholesalers sell and distribute prescription drugs to pharmacies for their
subsequent sale and dispensing to consumers. Wholesalers typically sell to pharmacies at
a mark-up on the WAC price that they pay to a manufacturer. Although business
agreements vary, WAC plus 2% is an amount commonly paid by pharmacies for brand
name prescription drugs.
Step 3
A publicly available pricing index known as AWP (Average Wholesale Price) is
established, for most brand name prescription drugs, by a direct mark-up of WAC. Two
companies, First Data Bank and Medispan, are the companies that publish AWP prices.
AWP serves as a prescription drug �sticker price�. It is used for relative price
comparisons and the reimbursement of pharmacies by insurers.
Prior to 2001, AWP was established as 120% of WAC.
In 2001, AWP for most brand name drugs was increased to 125% of WAC.
Step 4
Private and public payors of prescription drugs commonly use AWP as a reference point
for determining payment levels for pharmacy providers.For BRAND products
Based upon the Wholesale Acquisition Cost (WAC), which is the price that wholesalers pay to purchase the drug from the manufacturer. The WAC is marked-up by a fixed factor � typically 1.20 or 1.25 � to generate the AWP. Neither the determination of WAC nor the determination of AWP is subject to regulatory review.
Pharmaceutical companies make a prescription drug and assign it a price for sale in the
pharmacy distribution system, mostly through pharmaceutical wholesalers. The price is
referenced as Wholesale Acquisition Cost (WAC).
Step 2
Pharmaceutical wholesalers sell and distribute prescription drugs to pharmacies for their
subsequent sale and dispensing to consumers. Wholesalers typically sell to pharmacies at
a mark-up on the WAC price that they pay to a manufacturer. Although business
agreements vary, WAC plus 2% is an amount commonly paid by pharmacies for brand
name prescription drugs.
Step 3
A publicly available pricing index known as AWP (Average Wholesale Price) is
established, for most brand name prescription drugs, by a direct mark-up of WAC. Two
companies, First Data Bank and Medispan, are the companies that publish AWP prices.
AWP serves as a prescription drug �sticker price�. It is used for relative price
comparisons and the reimbursement of pharmacies by insurers.
Prior to 2001, AWP was established as 120% of WAC.
In 2001, AWP for most brand name drugs was increased to 125% of WAC.
Step 4
Private and public payors of prescription drugs commonly use AWP as a reference point
for determining payment levels for pharmacy providers.
5. Why AWP? Most common reference benchmark for pharmacy pricing
Developed in �60s to reimburse CA pharmacies for MediCal
Initially reflected pharmacy acquisition price from wholesaler
Over time, separation of AWP value from pharmacy acquisition price
PBMs adopted in �80s
Contractual reimbursement of prescription
Discounts expanded in relation to acquisition costs spread
80s: AWP �10%
90s: AWP �12%
00s: AWP �16%
6. Traditional AWP Discount Template Brand: Lesser of Pharmacy's Usual & Customary Price (retail price) or the Calculated price
Calculated Price = AWP -x% + dispense fee
Generic: Lesser of Pharmacy's Usual & Customary Price or the Calculated price
Calculated price = Lesser of:
MAC price + dispense fee or
AWP -x% + dispense fee
7. History: What happened to AWP? Lawsuit challenged determination of AWP prices
Amended settlement approved by US District Court (District of MA) for both First DataBank and Medispan
Reduced mark-up factor used in AWP to 1.20 times WAC or Direct Price
Approximately 1,400 NDCs specifically affected by settlement
Effective September 26, 2009
Independent of settlement
First DataBank & Medispan applied 1.20 mark-up to all other NDCs whose AWP is based on mark-up to WAC or Direct Price in excess of 1.20
Approximately 21,600 NDCs affected on September 26, 2009
Not affected: NDCs where manufacturers provide AWP to pricing compendia
Discontinuation of publication of AWP within 2 years [recently revised!]
Value of AWP unit cost prices decreased (roll-back!) The Allegations and Settlement
The lawsuits alleged that one of the major publishers of drug pricing information (along with a drug manufacturer) fraudulently colluded to increase the published AWP of over 400 brand drugs (affecting 1,442 individual National Drug Codes) by 5 percent from late 2001 to 2005. The suits also alleged that a second publisher negligently published the same inflated AWP information.
As a pricing benchmark, the AWP is the basis on which most brand drugs are contractually reimbursed. Pharmacy benefit managers (PBMs) and drugstores typically purchase drugs on the basis of the WAC, and then in turn sell them to third party providers (e.g., insurance companies, union health and welfare benefit plans, employer sponsors of self-insured welfare benefit plans) and individual members on the basis of AWP.
Under the settlement, for the 400 brand name drugs involved in the suit, the publishers will roll-back the mark up between the WAC and AWP from1.25 to 1.20 on Saturday, September 26, 2009 (i.e., the date that is 180 days after the entry of the Final Order and Judgment). At the same time, independent of the settlement, the publishers have decided to apply the same 1.20 mark-up factor to all other National Drug Codes whose AWP is based upon a mark-up from WAC in excess of 1.20. The result of the rollback will be to reduce the AWP on all of those drugs.
Separate from the settlement, the publishers have decided to discontinue altogether the publishing of AWP information within two years after the rollback � although they will reportedly continue to publish other drug pricing information (e.g., WAC and direct price).
A Brief History of AWP
Introduced in the late 1960?s, AWP evolved as a means of standardizing prescription drug reimbursements for the California Medicaid Program. Prior to the establishment of AWP, pharmacies billed according to what each one charged for drugs, creating a system that was labor intensive and plagued by inconsistent pricing. The California Medicaid program began paying pharmacies a standardized price for each drug. Ultimately insurers and employers embraced the concept and AWP became a benchmark for drug pricing and contracting. It was not long before publishing AWP and other drug pricing data evolved into a business in its own right.
One publisher was First Data Bank. The firm, founded in 1977, surveyed pharmaceutical wholesaler companies to determine the list prices for drugs being sold to retail pharmacies. Using a proprietary process, FDB blended wholesaler list prices to create the �average wholesale price� or AWP associated with the package size of product, as identified by its national drug (NDC) code. Quickly, AWP became the basis of the costs that third party payors incurred for drug products. In 1998, FDB acquired Medi-Span, a competing drug pricing compendia. Pricing established by FDB applied to both references until the FTC forced the sale of Medispan by FDB.
AWP Litigation
From its inception, FDB described the AWP as a value calculated from a survey of wholesaler prices. This was widely accepted to be the case until investigations for the class action suit revealed that since at least 20012 only the prices of one wholesaler, McKesson, were collected and reported. In late 2001 and early 2002, McKesson changed its methodology for drug pricing for approximately 1400 NDC codes. Historically, wholesalers varied their drug mark-ups, applying a 20% increase over wholesale acquisition cost (WAC) to some manufacturers? products while others were increased at 25%. McKesson adopted a 25% mark-up for many popular medications that were previously increased only 20%. Because McKesson was the sole source of wholesaler prices in FDB?s surveys, the action by McKesson raised AWP drug prices immediately. The Allegations and Settlement
The lawsuits alleged that one of the major publishers of drug pricing information (along with a drug manufacturer) fraudulently colluded to increase the published AWP of over 400 brand drugs (affecting 1,442 individual National Drug Codes) by 5 percent from late 2001 to 2005. The suits also alleged that a second publisher negligently published the same inflated AWP information.
As a pricing benchmark, the AWP is the basis on which most brand drugs are contractually reimbursed. Pharmacy benefit managers (PBMs) and drugstores typically purchase drugs on the basis of the WAC, and then in turn sell them to third party providers (e.g., insurance companies, union health and welfare benefit plans, employer sponsors of self-insured welfare benefit plans) and individual members on the basis of AWP.
Under the settlement, for the 400 brand name drugs involved in the suit, the publishers will roll-back the mark up between the WAC and AWP from1.25 to 1.20 on Saturday, September 26, 2009 (i.e., the date that is 180 days after the entry of the Final Order and Judgment). At the same time, independent of the settlement, the publishers have decided to apply the same 1.20 mark-up factor to all other National Drug Codes whose AWP is based upon a mark-up from WAC in excess of 1.20. The result of the rollback will be to reduce the AWP on all of those drugs.
Separate from the settlement, the publishers have decided to discontinue altogether the publishing of AWP information within two years after the rollback � although they will reportedly continue to publish other drug pricing information (e.g., WAC and direct price).
A Brief History of AWP
Introduced in the late 1960?s, AWP evolved as a means of standardizing prescription drug reimbursements for the California Medicaid Program. Prior to the establishment of AWP, pharmacies billed according to what each one charged for drugs, creating a system that was labor intensive and plagued by inconsistent pricing. The California Medicaid program began paying pharmacies a standardized price for each drug. Ultimately insurers and employers embraced the concept and AWP became a benchmark for drug pricing and contracting. It was not long before publishing AWP and other drug pricing data evolved into a business in its own right.
One publisher was First Data Bank. The firm, founded in 1977, surveyed pharmaceutical wholesaler companies to determine the list prices for drugs being sold to retail pharmacies. Using a proprietary process, FDB blended wholesaler list prices to create the �average wholesale price� or AWP associated with the package size of product, as identified by its national drug (NDC) code. Quickly, AWP became the basis of the costs that third party payors incurred for drug products. In 1998, FDB acquired Medi-Span, a competing drug pricing compendia. Pricing established by FDB applied to both references until the FTC forced the sale of Medispan by FDB.
AWP Litigation
From its inception, FDB described the AWP as a value calculated from a survey of wholesaler prices. This was widely accepted to be the case until investigations for the class action suit revealed that since at least 20012 only the prices of one wholesaler, McKesson, were collected and reported. In late 2001 and early 2002, McKesson changed its methodology for drug pricing for approximately 1400 NDC codes. Historically, wholesalers varied their drug mark-ups, applying a 20% increase over wholesale acquisition cost (WAC) to some manufacturers? products while others were increased at 25%. McKesson adopted a 25% mark-up for many popular medications that were previously increased only 20%. Because McKesson was the sole source of wholesaler prices in FDB?s surveys, the action by McKesson raised AWP drug prices immediately.
8. Effect of AWP Calculation Change Multiple �solutions� developed
Revising AWP discounts across the board to offset impact of price rollbacks
Brands
Generics: no change due to MAC
Establishing PBM-based pseudo AWP, using methodology similar to current AWP
Keep previous mark-up factor in place for each NDC
Lacks transparency
Alternative price benchmarks
No Change
Mostly state Medicaid programs; pharmacies took a haircut Method one is to reduce the discount off of AWP for brand products to pharmacies by 4 percent, which is the reduction of the value of AWP due to the actions taken by Medispan.�Navitus has determined that this a short-term solution since Medispan has announced that it will eliminate the publication of AWP within two years.
Method two is to apply a mark-up factor to the WAC price received by Medispan each week with the same mark-up factor as was available to the NDC prior to September 26, 2009.�In essence, this solution creates its own AWP.�This solution has some merit, as it allows for the existing contracts to continue without recontracting; and it is a change in definition of AWP.�There are two major drawbacks, however.�First, a system must be developed to mark up each WAC on each NDC that changes each week.�Secondly, this solution is not transparent but it maintains the status quo.
Method three is to convert to a WAC pricing algorithm. Navitus has calculated the relative discount off of AWP to a premium over WAC that will price drugs at the same amount.�This solution is both transparent and long term. WAC is provided to Medispan by the manufacturers and, therefore, is a widely published price point for pricing purposes.
Method one is to reduce the discount off of AWP for brand products to pharmacies by 4 percent, which is the reduction of the value of AWP due to the actions taken by Medispan.�Navitus has determined that this a short-term solution since Medispan has announced that it will eliminate the publication of AWP within two years.
Method two is to apply a mark-up factor to the WAC price received by Medispan each week with the same mark-up factor as was available to the NDC prior to September 26, 2009.�In essence, this solution creates its own AWP.�This solution has some merit, as it allows for the existing contracts to continue without recontracting; and it is a change in definition of AWP.�There are two major drawbacks, however.�First, a system must be developed to mark up each WAC on each NDC that changes each week.�Secondly, this solution is not transparent but it maintains the status quo.
Method three is to convert to a WAC pricing algorithm. Navitus has calculated the relative discount off of AWP to a premium over WAC that will price drugs at the same amount.�This solution is both transparent and long term. WAC is provided to Medispan by the manufacturers and, therefore, is a widely published price point for pricing purposes.
9. Effect of AWP Calculation Change (continued) Fractionation of the industry
Confusion
Which AWP is referenced?
Difficult to compare pricing between entities
Opportunity for certain entities to achieve additional margin Method one is to reduce the discount off of AWP for brand products to pharmacies by 4 percent, which is the reduction of the value of AWP due to the actions taken by Medispan.�Navitus has determined that this a short-term solution since Medispan has announced that it will eliminate the publication of AWP within two years.
Method two is to apply a mark-up factor to the WAC price received by Medispan each week with the same mark-up factor as was available to the NDC prior to September 26, 2009.�In essence, this solution creates its own AWP.�This solution has some merit, as it allows for the existing contracts to continue without recontracting; and it is a change in definition of AWP.�There are two major drawbacks, however.�First, a system must be developed to mark up each WAC on each NDC that changes each week.�Secondly, this solution is not transparent but it maintains the status quo.
Method three is to convert to a WAC pricing algorithm. Navitus has calculated the relative discount off of AWP to a premium over WAC that will price drugs at the same amount.�This solution is both transparent and long term. WAC is provided to Medispan by the manufacturers and, therefore, is a widely published price point for pricing purposes.
Method one is to reduce the discount off of AWP for brand products to pharmacies by 4 percent, which is the reduction of the value of AWP due to the actions taken by Medispan.�Navitus has determined that this a short-term solution since Medispan has announced that it will eliminate the publication of AWP within two years.
Method two is to apply a mark-up factor to the WAC price received by Medispan each week with the same mark-up factor as was available to the NDC prior to September 26, 2009.�In essence, this solution creates its own AWP.�This solution has some merit, as it allows for the existing contracts to continue without recontracting; and it is a change in definition of AWP.�There are two major drawbacks, however.�First, a system must be developed to mark up each WAC on each NDC that changes each week.�Secondly, this solution is not transparent but it maintains the status quo.
Method three is to convert to a WAC pricing algorithm. Navitus has calculated the relative discount off of AWP to a premium over WAC that will price drugs at the same amount.�This solution is both transparent and long term. WAC is provided to Medispan by the manufacturers and, therefore, is a widely published price point for pricing purposes.
10. ExampleAWP Roll-Back
11. Restatement of AWP Discount Many PBMs chose this method for brand products
Reduce AWP discount to reflect lower AWP values
Inconsistent discount factors between PBMs
Methodology to restate discount varied
Algebraic factor
Universal factor of 1.0417 (1.25/1.20) applied to brand discounts
Post Sept 2009 discount = ((1-Pre-Sept discount)*1.0417)-1
Factor based upon claims utilization
Book of business utilization
Client / Pharmacy specific utilization
Factor changes over time!
Change event reset �normal� expected discounts
What happens if AWP ceases to exist?
Variability to compare �discounts� between programs
12. Pseudo AWP Solution put forward by some PBMs
Higher PBM AWP values than published AWP values
Allowed existing AWP discounts to continue
AWP discounts are deeper than restated discounts; Net effect is similar
Two methodologies exist
All brand NDCs marked up by 125% WAC
Regardless of previous history
Each NDC is evaluated individually to determine its historical mark-up spread
Very complex to administer
Short term solution
New brand NDC AWPs history start at 120% WAC
Not Transparent!
AWPs are not published by national price compendia
13. Alternatives to Use of AWP?
14. Alternative Price Benchmarks Ideal Attributes
Widely Available
Potential for Longevity
Standardized
Stable
Reliable
Reported at a National Level
Transparent With the impending change in pricing methodology as of September 26th, 2009, Navitus prefers an alternate reimbursement methodology that�is widely available, long-term, standardized and reported at the national level. It has the best potential for longevity and will provide for stability, reliability and conforms to our mission of transparency. Wholesale acquisition cost is widely published and is a value that is provided to Medispan directly by the manufacturers of each product.With the impending change in pricing methodology as of September 26th, 2009, Navitus prefers an alternate reimbursement methodology that�is widely available, long-term, standardized and reported at the national level. It has the best potential for longevity and will provide for stability, reliability and conforms to our mission of transparency. Wholesale acquisition cost is widely published and is a value that is provided to Medispan directly by the manufacturers of each product.
15. Benchmark Solutions? Alternate Benchmark Price (ABP)
Average Manufacturer Price (AMP)
Average Selling Price (ASP)
Average Acquisition Cost (AAC)
True Acquisition Cost (Cost Plus)
Wholesale Acquisition Cost (WAC)
Don�t forget, Maximum Allowable Cost (MAC) Medi-Span is publishing an alternative benchmark, called the �Average WAC Pricing File�.� The concept is likely to meet with resistance as the industry is likely to view another publisher generated price index with suspicion. The product is being promoted as a means of offering clients pricing and contracting alternatives. Additionally, Medi-Span is promoting several other alternatives to clients. These include a subscription to a service which generates another calculated price, like the Average Average Wholesale Price, (AAWP) based upon the WAC. Another for generics is considered similar to the Generic Equivalent Average Prices (GEAP) known as the Generic Equivalent Wholesale Acquisition Cost (GEWAC). The publisher appears to be promoting this concept as an alternative to WAC pricing, particularly for those generic NDCs without a WAC, as (manufacturers may opt not to publish a WAC for certain drugs.) Medi-Span is publishing an alternative benchmark, called the �Average WAC Pricing File�.� The concept is likely to meet with resistance as the industry is likely to view another publisher generated price index with suspicion. The product is being promoted as a means of offering clients pricing and contracting alternatives. Additionally, Medi-Span is promoting several other alternatives to clients. These include a subscription to a service which generates another calculated price, like the Average Average Wholesale Price, (AAWP) based upon the WAC. Another for generics is considered similar to the Generic Equivalent Average Prices (GEAP) known as the Generic Equivalent Wholesale Acquisition Cost (GEWAC). The publisher appears to be promoting this concept as an alternative to WAC pricing, particularly for those generic NDCs without a WAC, as (manufacturers may opt not to publish a WAC for certain drugs.)
16. AWP Alternatives Alternate Benchmark Price (ABP) Published by FDB
Mimics the mark-up factor for the pre-September 2009 calculation of AWP
125% WAC
Not universally available
17. AWP AlternativesAverage Manufacturer Price (AMP) Potential long-term viable solution
Price based on actual manufacturer sales to wholesalers, pharmacies, others�In existence since early 1990�s
Used by CMS in Medicaid program for rebate calculations and as one component to calculate 340B prices
AMP unit price calculation changed with Healthcare reform
Not published, yet
Untimely updates
AMP prices calculated two quarters in arrears
Transparent, if published
Prices are on file with CMS
AMP files are used by CMS in the Medicaid program, these files are not currently available for public use. The publications,, which should have been released as a result of the Medicare Modernization Act, have not been made public. Publication of the price reference, which should have occurred as a result of Medicare Modernization Act, has been contested by drug manufacturers, pharmacies and wholesalers, in part because there�s disagreement on how AMP is defined. At issue for this proposal is that AMP is defined as the price wholesalers pay manufacturers for drugs to be distributed through �the retail class of trade.� This definition is critical because as currently defined by CMS, this class of trade includes PBM and mail order pharmacies, Medicaid, Medicare Part D, the State Children�s Health Insurance Program (SCHIP,) and the State Pharmaceutical Assistance Program. Opponents charge that the AMP calculation includes many transactions that have nothing to do with prices paid to wholesalers for drugs distributed to retail pharmacies. Interestingly, the hospitals, long term care pharmacy, federal supply schedule and prompt pay discounts aren't included in the AMP calculation.6 As is evident, the issue of using AMP is controversial from the outset. As a result, although it may be a valuable price standard, it is unlikely AMP will be accepted and available as a pricing benchmark in the near term. AMP files are used by CMS in the Medicaid program, these files are not currently available for public use. The publications,, which should have been released as a result of the Medicare Modernization Act, have not been made public. Publication of the price reference, which should have occurred as a result of Medicare Modernization Act, has been contested by drug manufacturers, pharmacies and wholesalers, in part because there�s disagreement on how AMP is defined. At issue for this proposal is that AMP is defined as the price wholesalers pay manufacturers for drugs to be distributed through �the retail class of trade.� This definition is critical because as currently defined by CMS, this class of trade includes PBM and mail order pharmacies, Medicaid, Medicare Part D, the State Children�s Health Insurance Program (SCHIP,) and the State Pharmaceutical Assistance Program. Opponents charge that the AMP calculation includes many transactions that have nothing to do with prices paid to wholesalers for drugs distributed to retail pharmacies. Interestingly, the hospitals, long term care pharmacy, federal supply schedule and prompt pay discounts aren't included in the AMP calculation.6 As is evident, the issue of using AMP is controversial from the outset. As a result, although it may be a valuable price standard, it is unlikely AMP will be accepted and available as a pricing benchmark in the near term.
18. AWP AlternativesAverage Selling Price (ASP) Unit price used in Medicare Part B program
Limited scope of products
Injectables
DME
Published
Transparent
Untimely updates
ASP prices are calculated two quarters in arrears
Doesn�t reflect current market changes
19. AWP AlternativesAverage Acquisition Cost (AAC) Concept put forward by Alabama Medicaid�CMS RFP
Determine AAC by NDC through pharmacy wholesale invoice surveys�State can compel pharmacies to provide
Alabama reimburses pharmacy average cost by NDC + dispense fee (~$12)
Alabama publishes each NDC�s AAC on website
Applies to both brand and generic drugs
Not published nationally
Updates of AAC prices are not timely
Wholesale invoice prices may not be transparent
Pharmacies can manipulate wholesale invoices through subsidiaries
Scalable?
20. AWP AlternativesTrue Acquisition Cost (Cost Plus) Concept put forward by some pharmacies and available from some PBMs
Avoids spread issue inherent in AWP pricing
Pharmacy provides client/PBM with actual acquisition cost
Pharmacy reimbursed Cost Plus Dispense Fee
Dispense fee is true fee to cover administration, dispensing and profit
$8 - $12
Transparent, yet not
Concept is ideal
Better prices are passed directly through to the payer
Cost is not publicly available nor published
Requires extensive audits to confirm �cost� is truly net cost
Scalable?
Perhaps with limited network�mail vendors �cost plus� model. Wal-Mart and Caterpillar have moved forward with such a program and recently announced plans to expand the offering to several other companies.7 The concept is viewed favorably because it controls expenses and avoids the problems inherent in AWP based contracting. The potential issue with this approach is transparency. Certainly, invoice pricing might be used for a �cost,� but extensive auditing would be required to identify discounts that might be offered separately and in order to confirm that �cost� was truly based upon final cost. �cost plus� model. Wal-Mart and Caterpillar have moved forward with such a program and recently announced plans to expand the offering to several other companies.7 The concept is viewed favorably because it controls expenses and avoids the problems inherent in AWP based contracting. The potential issue with this approach is transparency. Certainly, invoice pricing might be used for a �cost,� but extensive auditing would be required to identify discounts that might be offered separately and in order to confirm that �cost� was truly based upon final cost.
21. AWP AlternativesWholesale Acquisition Cost (WAC) Viable benchmark available and used by PBMs today
Widely reported nationally by manufacturers and published by all pricing compendia
WAC: Manufacturer�s published list price to wholesalers (excluding applicable discounts)
Available for well over 99% of brand products
Approximately 85% of utilized generic products
Used in calculation of most brand AWP unit prices
Most transparent of current industry options
Determined and provided by manufacturers
Not manipulated by pricing compendia
Not manipulated by PBMs using AWP discount factors
Translating WAC to AWP discount requires experience
22. WAC �Discount� Template Brand: Lesser of Pharmacy's Usual & Customary Price (retail price) or the Calculated price
Calculated Price = WAC (plus or minus) x% + dispense fee
Generic: Lesser of Pharmacy's Usual & Customary Price or the Calculated price
Calculated price = Lesser of:
MAC price + dispense fee or
WAC (plus or minus) x% + dispense fee or
AWP -x% + dispense fee
23. WAC Reimbursement ExampleBrand Aciphex (quantity of 30)
U&C submitted by pharmacy = $185.00
WAC = $5.70433/unit x 30 = $171.13 + 5% = $179.69 + $1.50 df = $181.19
AWP (current) = $7.13044/unit x 30 = $213.91 -16% = $179.69 + $1.50 df = $181.19
AWP (new) = $6.84520/unit x 30 = $205.36 -16% = $172.50 + $1.50 df = $174.00
24. Industry Translation of �Discounts� AWP change event created more chaos
No more �apples to apples�
Widely variable AWP �discounts� in RFPs � what�s real?
Payers / Consultants must demand transparency
Ask how discount determined
Ask how AWP determined
Ask for alternate benchmarks to triangulate discounts
PMPM drug costs expected to be incurred by Payer
True evaluation between programs
Could be �apples to apples� comparator among differing benchmarks
25. Questions?
26. Thank you�