Download
1 / 36
360 likes | 515 Views
Atherosclerosis. Dr. Gerrard Uy. Definition. Also known as arteriosclerotic vascular disease condition in which an artery wall thickens as a result of the accumulation of fatty materials such as cholesterol. Pathogenesis.

E N D
Atherosclerosis Dr. GerrardUy
Definition • Also known as arteriosclerotic vascular disease • condition in which an artery wall thickens as a result of the accumulation of fatty materials such as cholesterol
Pathogenesis • Remians the major cause of death an premature disability in developed societies • Predisposed areas for atherosclerosis: • Proximal left anterior descending artery • Proximal portion of the renal artery • Carotid bifurcation
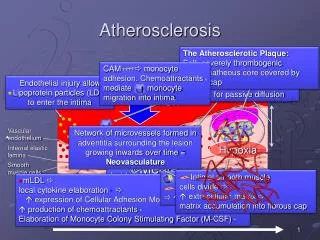
Initiation of Atherosclerosis • Initial lesion is the fatty streak
Initiation of Actherosclerosis • Accumulation of leukocytes characterizes the formation of early atherosclerotic lesion • Once resident within the initma, the macrophages become lipid laden foam cells • Not all fatty streaks progress to form complex atheromata • Depends on the activity of the macrophage • The amount of lipid entering the artery • Reverse cholesterol transport
Initiation of Actherosclerosis • As atherosclerotic lesions advance, abundant microvessels develop within the artery
Major Risk Factors that Modify LDL Goals • Cigarette smoking • Hypertension (BP>140/90 mmhg) • Low HDL (<40 mg/dl) • Diabetes mellitus • Family hx of premature coronary heart disease • Age (men>45, women>55 yrs) • Life style risk factors • Obesity (>30kg/m2) • Physical inactivity • Atherogenic diet
Ischemic Heart Disease Dr. GerrardUy
Definition • A condition in which there is an inadequate supply of blood and oxygen to a portion of the myocardium • Occurs when there is an imbalance between myocardial oxygen supply and demand
Epidemiology • Most common, serious, chronic, life threatening illness in the United States • High fat and energy rich diet, smoking and sedentary lifestyle are associated with the emergence of IHD • Obesity, insulin resistance, and diabetes are powerful risk factors for IHD
Pathophysiology • Major determinants of myocardial oxygen demand: • Heart rate • Myocardial contractility • Myocardial wall tension • Adequate supply of oxygen requires a satisfactory level of oxygen carrying capacity of the blood and adequate level of coronary blood flow
Coronary Atherosclerosis • Epicardial coronary arteries are the major site of atherosclerotic disease • Predilection for atherosclerotic plaques to develop at sites of increased turbulence in coronary flow • Location of the obstruction influences the quantity of the myocardium rendered ischemic • The severity and duration determine if the damage is reversible (< 20 mins for total occlusion in the absence of collaterals) or permanent (> 20 mins)
Stable Angina Pectoris • Due to transient myocardial ischemia • Males constitute ~70% of all patients with angina pectoris • Characteristics: • Chest pain (squeezing, heaviness, smothering, etc) • Poorly localized chest pain (Levine’s sign) • Crescendo – decrescendo pattern • Lasts 2 – 5 mins • Can radiate to either shoulder and to both arms, back root of the neck, jaw, teeth, and epigastrium • Typically caused by exertion and relieved by rest or sublingual nitroglycerin
Stable Angina Pectoris • Anginal equivalents: • Dyspnea • Nausea • Fatigue • faintness • The history of typical angina pectoris establishes the diagnosis of IHD until proven otherwise
Stable Angina Pectoris • Physical Examination: • Often normal in patients with stable angina pectoris when they are asymptomatic • Laboratory examination: • CBC • Urinalysis • Lipid Profile • FBS • Creatinine • CXR • 12 L ECG • Stress testing • Cardiac imaging
Stable Angina Pectoris • Management plan: • Explanation and reassurance • Identification and treatment of aggravating factors • Adaptation of activity • Treatment of risk factors • Drug therapy • Nitrates • B blockers • Ca channel blockers • Anti platelets
Unstable Angina and Non ST Elevation Myocardial Infarction Dr. GerrardUy
Unstable Angina • Diagnosis of of UA is based largely on the clinical presentation • Characteristics: • Chest discomfort with at least one of three features • Occurs at rest (or with minimal exertion) • Lasts > 10 mins • Severe and of new onset (within the prior 4-6 weeks) • Crescendo pattern
Pathophysiology • Plaque rupture or erosion with superimposed non occlusive thrombus – most common cause • Dynamic obstruction (coronary spasm) • Progressive mechanical obstruction • Secondary unstable angina
Clinical Presentation • Clinical hallmark of NSTEMI is chest pain located in the substernal region • ECG shows ST segment depression, T wave inversion • Cardiac biomarkers are elevated
Management • Medical treatment (complete bedrest with continuous ECG monitoring) • Anti-ischemic treatment • Nitrates • B blockers • Anti-thrombotic • Aspirin • clopidogrel
ST Segment Elevation Myocardial Infarction Dr. GerrardUy
one of the most common diagnoses in hospitalized patients • mortality rate from AMI is ~30% • more than half of these deaths occurring before the stricken individual reaches the hospital • Mortality is approx 4 fold higher in elderly patients compared with younger patients
Acute STEMI • usually occurs when coronary blood flow decreases abruptly after a thrombotic occlusion of a coronary artery previously affected by atherosclerosis • occurs when a coronary artery thrombus develops rapidly at a site of vascular injury • Injury facilitated by factors such as cigarette smoking, hypertension, and lipid accumulation
Pathogenesis • Atherosclerotic plaque disruption • Thrombogenesis • Platelet activation • Platelet aggregation, cross-linking • Coagulation cascade activated
The amount of myocardial damage depends on: • the territory supplied by the affected vessel • whether or not the vessel becomes totally occluded • the duration of coronary occlusion • the quantity of blood supplied by collateral vessels to the affected tissue • the demand for oxygen of the myocardium whose blood supply has been suddenly limited • native factors that can produce early spontaneous lysis of the occlusive thrombus • the adequacy of myocardial perfusion in the infarct zone when flow is restored in the occluded epicardial coronary artery.
Risk factors • Persons with multiple coronary risk factors • Persons with unstable angina • Hypercoagulability • collagen vascular disease • cocaine abuse • intracardiac thrombi or masses that can produce coronary emboli
Clinical presentation • In up to ½ of cases, a precipitating factors appears to be present • Usually soon after awakening • PAIN – most common presenting complaint • Deep, visceral • Heavy, squeezing, crushing, stabbing, burning • Similar to angina pectoris but occurs at rest • No relief from rest • More severe, lasts longer • Central portion of chest/ epigastrium/ radiates to arm • weakness, sweating, nausea, vomiting, anxiety, and a sense of impending doom
PE Findings • anxious and restless • Pallor, perspiration • Combination of substernal chest pain persisting >30 mins and diaphoresis strongly suggest STEMI • physical signs of ventricular dysfunction • fourth and third heart sounds, decreased intensity of the first heart sound, and paradoxical splitting of the second heart sound
Lab Findings • Electrocardiogram (ECG) • ST-segment elevation • Serum Cardiac Biomarkers • Proteins released from necrotic heart muscle • Troponin I • CKMB • Cardiac imaging
Management • Prehospital care • Recognition of symptoms • Rapid deployment of medical team • Expeditious transportation • Implementation of reperfusion therapy • ER management • Control of discomfort • Limitation of infarct size • O2
Intervention • Primary percutaneous coronary intervention • Angioplasty • Applicable to patients who have contraindications to fibrinolysis • Fibrinolysis • Within 30 mins of presentation • tPA • Streptokinase • rPA (reteplase)
Hospital care • Should be admitted in the CCU or ICU • Bed rest for first 12 hours • Resume upright position with dangling feet within 24 hours • NPO in first 4-12 hours • 50-55% CHO, <30% fats, cholesterol < 300 mg/dl • Bedside commode, laxative • Sedation (diazepam)