Download

1 / 35
480 likes | 1.26k Views
Pneumothorax. MR 8/17/09 J.Chen. Chest Pain. Differential Diagnosis Musculoskeletal Cardiac Gastrointestinal Respiratory Psychogenic Miscellaneous. Musculoskeletal. Chest Wall Strain Costochondritis Direct Chest truama. Cardiac. Arryhthmia SVT PVC Coronary Artery Aneurysm

E N D
Pneumothorax MR 8/17/09 J.Chen
Chest Pain • Differential Diagnosis • Musculoskeletal • Cardiac • Gastrointestinal • Respiratory • Psychogenic • Miscellaneous
Musculoskeletal • Chest Wall Strain • Costochondritis • Direct Chest truama
Cardiac • Arryhthmia • SVT • PVC • Coronary Artery Aneurysm • Infection • Myocarditis • Pericarditis • Myocardial Infarction/Ischemia • Structural abnormalities • Aortic Stenosis • Hypertrophic Cardiomyopathy • PulmonicStenosis • Mitral Valve Prolapse • Severe Coarctation of the aorta
Gastrointestinal • Caustic Ingestion • Esophageal foreign body • Esophagitis • GERD
Respiratory • Asthma • Cough • Pleural Effusion • Pneumonia • Pneumothorax • Pneumomediastinum • Pulmonary Embolism
Psychogenic • Anxiety • Hyperventilation
Miscellaneous • Breast Mass • Shingles • Sickle Cell Crisis • Thoracic Tumor
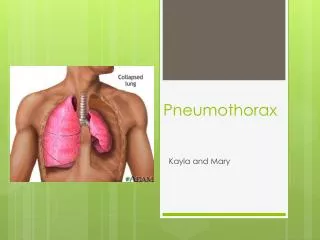
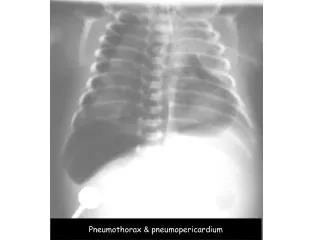
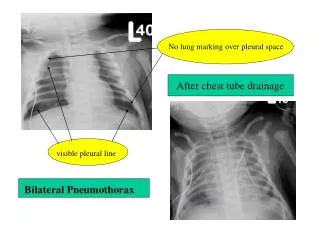
Pneumothorax • Presence of air between the visceral and parietal pleura that leads to lung collapse
Pneumothorax • Traumatic • Iatrogenic • Spontaneous • Primary • Secondary
Traumatic Pneumothorax • Penetrating Trauma (eg Bullet, Knife) • Air entering pleural space directly through chest wall • Blunt Trauma • Rib Fracture • Alveolar rupture from sudden compression • High Risk Occupations • Diving • Flying
Iatrogenic Pneumothorax • Transthoracic Needle Aspiration biopsy • Transbronchial Biopsy • Thracentesis • Central Venous Catheter Placement • Intercostal Nerve Block • Tracheostomy • CPR • Positive Pressure Ventillation • NG tube placement
Spontaneous Pneumothorax • Due to rupture of apical Blebs • PSP-Pt do not have clinically apparent lung disease • Subpleural bullae found in 76-100% of patients undergoing VATS
Risk Factors-PSP • Smoking • Tall, Thin stature • Marfan • Birt-Hogg Syndrome-AD, characterized by benign skin tumors, renal/colon cancer, Sp PTX • Pregnancy • Familial PTX
Conditions Associated with SSP • Chronic Obstructive Lung Disease • Asthma • Tuberculosis • Cystic Fibrosis • Marijuana, Cocaine • HIV/AIDS with PCP infection • Necrotizing PNA • Bronchogenic Carcinoma • Metastatic Malignancy • Sarcoidosis • Idiopathic Pulmonary Fibrosis • ARDS
History • Usually occur while at rest • Acute onset of chest pain • Severe • Stabbing • Radiates to ipsilateral shoulder • Pleuritic • Sudden onset of SOB • Anxiety • Cough • Dyspnea
Physical Exam • Vital Signs: • Tachypnea • Tachycardia • Hypotension • Hypoxia • PulsusParadoxus • General Appearance • Diaphoretic • Splinting • Cyanotic
Physical Exam • Respiratory • Decreased Breath Sounds • Hyperresonance to percussion • Decreased Tactile Fremitus • “Scratch Sign” • Cardiovascular • JVD • Shift in PMI • Other • Subcutaneous Emphysema • Shifted Trachea • Altered Mental Status
Laboratory Studies • ABG • PO2 frequently decreased • Increased A-a gradient • PCO2: • Elevated with respiratory compromise • Decreased from Hyperventilation
Imaging • CXR-confirmatory • CT • Useful for finding small pneumothoraces • Distinguish PTX from bleb or cyst • Locating small blebs • US • Increasing in use • 95%sensitivity, 100%specificity
Managment • Small PTX (<3cm): • Observation • High Flow O2 • No further management if CXR in 24 hr is small/stable
Management • Large PTX • Hospitalization • Chest tube +/- suction until lung reexpands and air leak resolves • Chemical Pleuredesis • Talc • Bleomycin, tetracycline, povidone iodine • Video Assisted Thorascopic Surgery (VATS) • Removal of Blebs • Surgical pleurodesis • Attach lung to intrathoracic chest wall • Mechanical abrasion of the lung
Recurrence rate based on intervention • Overall between 16-52%