Download
1 / 38
530 likes | 1.38k Views
PNEUMOTHORAX. Leszek Kutwin, Szymon Wcisło, Robert A. Stolarek. Anatomy. Pleural cavity is a bilateral serum space inside the chest limited by parietal pleura, lining chest walls and visceral pleura, lining lungs themselves. Anatomy.

E N D
PNEUMOTHORAX Leszek Kutwin, Szymon Wcisło, Robert A. Stolarek
Anatomy Pleural cavity is a bilateral serum space inside the chest limited by parietal pleura, lining chest walls and visceral pleura, lining lungs themselves
Anatomy • Pleura is made up of several strata of connective tissue covered with a single layer of mesothelial cells. • The visceral pleura may excrete substances leaking out from lung parenchyma. • The partial pleura can absorb substances from pleural cavity.
Physiology Under physiological conditions parietal and visceral pleura form capillary space 7 – 24 m wide, containing small amount of visceral fluid of approx. volume 0,1 – 0,2 ml/kg m.c.
Physiology • Pleural cavity plays important role in respiratory processes. • The size of the cavity and pressures inside affect lung, heart and large vessels • It is a site of absorption and excretion of fluids and substances inhaled into lungs. • The pleural fluid contains cells, proteins, lipids, enzymes and antigens.
Physiology • The elastic recoil of chest wall maintains negative pressure inside the thorax cavity and the constant expansion of the lungs. • During breathing this pressure is the lowest at the top of inhalation and the highest at the top of exhalation.
Physiology Mean pleural pressure is approx. 5 cm H2O, but during forced expiration and forced inspiration it may range from • – 54 cm H2O • + 70 cm H2O respectively.
Physiology • Further, there is a pressure gradient between lowest pressure at the top of pleural cavity and the highest at the base of pleural cavity. • This gradient is 0,5 cm H2O, what is in standing position related with an apex-base pressure gradient of up to 12 cm H2O.
Physiology Pneumothorax is the state of air invasion into pleural cavity. It is classified according to the following criteria: 1. the site of air invasion • Internal pneumothorax (via lung, bronchi, trachea, esophagus) • External pneumothorax (via thorax wall) 2. The communication between pleural cavity and the atmosphere • open • closed • Valve type (pressurized, ventilate)
Pathology 3. Pneumothorax etiology • spontaneous primary, without changes in the lungs • spontaneous secondary, with accompanying lung disease • non-iatrogenic traumatic (open, closed trauma) • iatrogenic traumatic (BAC, subclavic venosection, intercostal nerve blockage, aspiration of pleural fluid) 4. Pneumothorax size • complete • partial
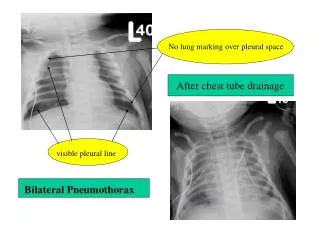
Pathology Pneumothorax size Based on chest X-ray the approximate size of pneumothorax can be determined. When the mean chest wall pleural distance is: • 1 cm, the approx. Pneumothorax size is 15% • 2 cm – 23% • 4 cm – 40% of thorax capacity.
Pathology Clinical symptoms • Chest pain radiating to shoulder at the site of pneumothorax • dyspnea • Evident percussion sound, restriction of range of movements and decrease ofalveolar sound on auscultation • Mediastinum shift towards non-affected site • In extreme conditions: hypoxia, hypercapnia, right-left blood shunt of deoxygenated blood from pulmonary circulation to the systemic circulation • Lung collapse verified with X-ray
Therapy It is related with : • pneumothorax type • its causes • symptomatic intensity • pneumothorax size
Therapy Therapeutic procedures in spontaneous pneumothorax • initial • The size below 15% of thorax cavity volume • Does not increase • Sometimes without clinical symptoms • In young persons • May be managed with pharmacotherapy The time of pneumothorax absorption is 1,25% of total capacity within a day. Patient is instructed: • To stay in bed • Perform appropriate respiratory exercises • Oxygen therapy (FiO2 = 0,4).
Therapy In patients with spontaneous pneumothorax larger than 15% and in symptomatic patients chest puncture and air aspiration out of the pleural cavity is required. The efficiency of this procedure is approx. 60%, whereas recurrence is estimated for 20-50%.
Therapy Inefficient therapy or the pneumothorax puncture, severe symptoms, pressurized and recurrent pneumothorax are the state requiring the drainage of pleural cavity and detailed diagnostic workup.
Therapy Management of secondary of pneumothorax • It is associated with numerous lung diseases (COPD, Tbc, neo, infection) and affect mainly elderly. • It is usually severe with marked dyspnea and the recurrence rate is about 40-50%. Therefore, the pleural drainage is an essential therapeutic option in this type of pneumothorax and it efficiency is estimated for 82%. • In secondary pneumothorax, drainage is aided with chemical pleurodesis and at the sustained air leak videothoracoscopy (VT) or toracotomy is considered.
Therapy Management of traumatic pneumothorax • It may be caused by blunt trauma or penetrating injury or it may be either iatrogenic and non-iatrogenic. • Minor size pneumothorax up to 15% may be managed with pharmacotherapy or aspiration biopsy. • The failed therapy with these options, pneumothorax recurrence, multiple costal fractures and scheduled intubation are contradictions of initial management of traumatic pneumothorax with drainage.
Therapy Initial mamagement • Open pneumothorax should always be changed into closed pneumothorax with the use of air tight opatrunki and then sucking drainage • The initial decrease of pleural pressure with the insertion of thick needle of 2,5 mm into 2nd intercostal space in the mamary line with cute rubber finger or fixed small drainage with outflow below the water surface
Therapy VT and toracotomy indications • The inefficiency of sucking drainage due to partial lung expension • Sustained continuous air leakage for 7-10 days • Rapid surgery due to massive leakage • Reccurent pneumothorax • X-ray confirmation of emphysematous bullae
Therapy The site of drainage insertion • II or III intercostal space in mammary line in case of pneumothorax • V or VI intercostal space inmaxiallary medial line in case of pneumothorax and fluid
Means of pleural drainage • They are build from: • Drainer and connectors • bottles • Vacuum device • Characteristics of pleural drainage tools • commonly made from PCV • do not display cytotoxic properties • Should not sensitize, hemolyze or coagulate blood • Flexible but still quite stiff • transparent • Lowest internal diameter 6 mm • incorporated X ray marker • Optimal adult drainage sytems 26 – 40 F (of 6-11mm internal diameter)
Means of pleural drainage • Two types of bottle systems include: • Passive drainage systems (gravity type) • Acitve drainage systems (sucking type) • Sucking devices are water based and vacuum based. The negative pressure must be higher than the late expiratory pleural pressure • In clinical setting vacuum does not exceed – 20 cm H2O
Means of pleural drainage Gravity drainage. The bottle has a reservoir and underwater vavle funtions.
Means of pleural drainage Single use drainage sets (plastics) • Pleurevac • Tucker GA. Atrium • Thoraklex • Thora Seal, Aqua Seal, Duble Seal Plastic sets are in the majority single use analogues similar to traditional systems.