Download
1 / 27
270 likes | 383 Views
Mathematical models for interventions on drug resistance. Hsien-Ho Lin. Motivation….

E N D
Mathematical models for interventions on drug resistance Hsien-Ho Lin
The first model builders in tuberculosis met with considerable opposition from those who maintained that many essential parameters were not established with sufficient precision, although paradoxically, those very opponents apparently had their own intuitive models on which to base highly assertive decisions. World Health Organization, 1973 cited by Lietman and Blower CID 2000
Which interventional strategies are possible? • Cycling • “Search and destroy” • Rapid diagnostic testing • Antibiotic restriction • Education interventions/campaigns • Antibiotic combinations • Short course/higher doses
How to choose between alternative strategies? • Requires: • Clearly stated goal(s) of control • A method to compare the ability interventions to meet these goals • How to compare the performance of interventions? • Observation • Quasi-experimental • Experiment / Clinical trials • Model
Challenges • Observational study • Baseline differences / Confounding • Individual / group level effect • Time trend / stage of epidemics • Clinical trial: randomized study • Long enough duration to detect delayed effects • Many possible interventions to be tested • Ethical limitations • Models
What is a model? • Simplified representation of a more complex system • Goal: • Develop a model which omits details which do not affect the behavior of the system • Model will reflect both the system studied and the question asked • Why create a model? • Complex systems are difficult to understand • We all use models, here we are formalizing
How do we decide what to omit? • Develop candidate model(s) which includes only those details that we think to be essential • for the natural history of disease • for the interventions we intend to simulate • Our knowledge of natural history and disease trends help determine parameter values and inform the structure of a model • but do not do so uniquely!
Case study I • Modeling the impact of antibiotic cycling
Fig. 1. Schematic diagram of the model and the corresponding differential equations β=1 c=0 γ=0.03 m=0.7 m1=.05 m2=.05 τ1+τ2=0.5 μ=0.1 σ=.25 α=0.8 Bergstrom, Carl T. et al. (2004) Proc. Natl. Acad. Sci. USA 101, 13285-13290
Fig. 3-4. Fraction of patients carrying resistant bacteria, for cycle lengths of 1 yr, 3 months, and 2 weeks, respectively Bergstrom, Carl T. et al. (2004) Proc. Natl. Acad. Sci. USA 101, 13285-13290
A bug’s view Bergstrom, Carl T. et al. (2004) Proc. Natl. Acad. Sci. USA 101, 13285-13290
Authors’ conclusion • Cycling is unlikely to be effective and may even hinder resistance control
Hm….. • Model structure • Mixed colonization? • Parameter values • Constant rate assumption • A strain never totally dies out • Homogeneous mixing
Case study II • Modeling the impact of “search and destroy” and rapid diagnostic testing
Fig. 1. Patient dynamics (a) and MRSA dynamics (b) within a hospital Bootsma, M. C. J. et al. (2006) Proc. Natl. Acad. Sci. USA 103, 5620-5625
Fig. 3. Effect of intervention strategies on nosocomial prevalence levels when isolation is 100% effective Bootsma, M. C. J. et al. (2006) Proc. Natl. Acad. Sci. USA 103, 5620-5625
Fig. 4. Changes in critical reproduction ratio (R0c) for several combinations of intervention measures according to changes in model parameters Bootsma, M. C. J. et al. (2006) Proc. Natl. Acad. Sci. USA 103, 5620-5625
Authors’ conclusions • …… • MRSA-prevalence can be reduced to <1% (within 6 years) in high-endemic settings by S&D • ….. • RDT can reduce isolation needs by >90% in low-endemic settings and by 20% in high-endemic settings • ???
Challenges for developing models for assessing interventions for drug resistance “…as we know, there are known knowns; there are things we know we know. We also know there are known unknowns; that is to say we know there are some things we do not know. But there are also unknown unknowns -- the ones we don't know we don't know." Donald Rumsfeld Former US Secretary of Defense
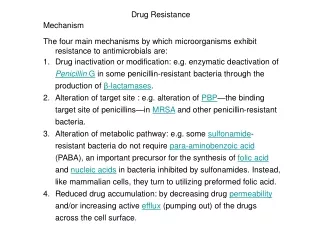
Known knowns • Colonization occurs after exposure to colonized patients • A hospital is an open system • People can enter a hospital colonized with the pathogen of interest • Antibiotics used at a much higher rate in the hospital • Spontaneous clearance of colonization
Known unknowns • Fitness cost of being resistant • Supercolonization • Importance of mixed colonization; within-host competition between strains under different scenarios of selection pressure • Details of transmission where assumptions of homogeneity break down • Unanticipated human, pathogen, environmental behavior • What changes will occur as epidemic progresses and interventions are implemented?
Unknown unknowns • Unanticipated consequences of interventions • Synergistic • Antagonistic
Caveat • We should expect that the lists of known unknowns and unknown unknowns are longer than the first list • Should give us pause about our ability to accurately project disease trends into the future
Conclusions • We need models to help form interventional strategies against antibiotic resistance (we have few reasonable alternatives) • These models reflect both our knowledge and ignorance of the essential processes underlying the transmission dynamics of pathogens within hospitals/communities • These models will inform us of the most important areas for further research • These models should allow us to rank categories of interventions in their probable impact on our chosen outcome • However, precise quantification of impact of interventions is too much to ask of these crude tools