Download
1 / 39
390 likes | 573 Views
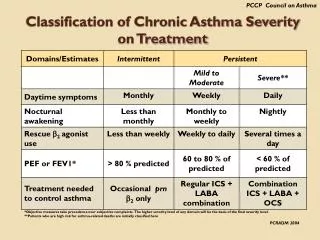
Studies of Chronic Aspiration GERD Associated Asthma. Asthma Chronic inflammatory disease Recurrent respiratory symptoms, wheezing, breathlessness, chest tightness, coughing, Increase airway mucus secretion Increase smooth muscle hyper-reactivity

E N D
Studies of Chronic Aspiration GERD Associated Asthma
Asthma Chronic inflammatory disease Recurrent respiratory symptoms, wheezing, breathlessness, chest tightness, coughing, Increase airway mucus secretion Increase smooth muscle hyper-reactivity Inflammatory cells involved: T lymphocyte, eosinophil, mast cells, epithelial cells
Risk Factors Disease inception: viral infection Enviromental exposure: allergen, pollution, tobacco smoke Life style: living on farm, diet, antibiotic use Comorbid condition: atopic dermis, obesity
Excerbating Factors Allergens: Mites, trees, grasses, animal danger → chronic low level exposure to indoor allergens ( house dust ,cockaroach , Alternaria species) ► fur pet exposure reduce future risk ► pollen immunotherapy in school age also reduce future risk
Infections Chlamydis , Mycoplasma, Early childhood inceltion, infection of virus in established asthma Exercise Causing airway obstruction, bronchoapasm
Non steroid anti-inflammatory drug →the response to aspirin or NSAIDS , eve laceimation, severe bronchospasm →reduced prostaglandin production for normal lung function • Psychological factors →Parental stress Gastroesophageal reflux( GERD) • → 45-60% of adult and children with asthma has • GERD • → microaspiration or irritation of esophagus with • reflux bronchispasm
Enviroment Genetic desposition Normal airway function Asthma remodeling injury Epithelial injury repair angiogenesis Matrix deposition Genetic predisposition for remodeling
GERD( Gastro Esophageal Reflux Disease) recurrent return of stomach content back up into the oesophagus 10% of pateirts with GERD develop Barrett’s oesphagus which increases the risk of cancer of the oesophagus 80% of patients with GERD also have a hiatal hernia
Theory proposed for pathophysiologic mechanism of GERD associated Asthma Direct stimulation of airway inflammation by aspiration of gastric contents or airway hyperresponsiveness triggered by aspiration of minute amounts of acid into the lower airway Gastric Fluid Acid Food allergen digestive enzyme may promote inflammaion of airway and smooth muscle tissue
Airway Remodeling Subepithelial fibrosis, myofibroblast hyperplasia, myocyte hyperplasia and hypotrophy Epithelial damage Globet cell metaplasia oedema
Innate Immunity • Provide initial protection against microorganism infection • Cellular components of innate immunity: • neutrophil, macrophage and natural killer cells • Major target of innate immune response are pathogen associated molecules pattern( PAMP) • Recognize microorganism through germline-encoded pattern recognition( PRRs)
Mammalian Immune response Innate immunity: first line of host defense against pathogen, and mediated by phagocytes include macrophage and dendritic cells Acquired immunity: Characterized bt specificity and develops by clonal selectionfrom lymphocytesbearing antigen –specific receptors that are generated through gene rearrangement
PAMP • molecule structure that are produced only by microbial pathogen • conserved molecule pattern that are essential for the survival of the microbes • shared by large groups of micro organisma • often represent molecule signature of microbes, i.e. LPS
PRRs • Recognize PAMP which is essential for the survival of • microorganisms • Express constitutively in the host cells • Germline encoded, nonclonal, express on all cells of a given type, and independent of iminologic memory
TLR( Toll Like receptors) A pattern recognition receptor Highly preserved from Drosophilla to mammals Toll : gene essential for fly dorsal ventral development Induction immune-response to broad range of pathogens: virus, bacteria, fungus, protozoa, helminths ROS( reactive oxygen species), products of cell damage or cell death
Toll receptors and their ligands Poly(I-C) d.s. RNA Lipoprotein, Gram positive, mycobacterial cell wall constituents Imiguimoid Resiquimod 848 Gram negative bacterial LPS, HSP, fibrinogens CpG DNA ? Flagellin TLR9 TLR10 TLR7 TLR8 TLR5 TLR4 TLR3 TLR1/ TLR2 TLR2/ TLR6
TIRAP ubc13 Uev1A TRAM TRAF6 IRF-5 NEMO/IKK TRAF6 IKK- IKK- Ubk63 TAB1 TAK1 TAB2 IKK complex IKK-I TBK1 NF-κB JNK P38 UbK48 P NF-κB P IRF-3 p p IRF-3 AP-1 NF-κB IRF-5 TLR-signaling pathway IL-1R MyD88 TLR4
TLR4 MyD88 IRAK-1 IRAK-4 TLR-signaling pathway IL-1R
MyD88 IRAK-1 IRAK-4 TRAF6 IRF-5 Ubk63 ubc13 UbK48 IB Uev1A TAB1 NEMO/IKK Pi TAK1 TAB2 Ubk63 IKK- IKK- JNK P38 AP-1 NF-κB IKK complex P P IRF-5
TLR4 TRAM TRAF6 IKK-i TBK1 RIP1 NF-κB p IRF-3
The potentials of TLRs to influence respiratory disease Activation of neutrophilic and monocytic inflammation Protective immunity septic shock TLR activation Asthma Activation Cytokine production Th1/2 biasing COPD (chronic obstructive pulmonary disease) ARDS (acute respiratory distress syndrom) DC/T cell Clearance of infection Bronchiolitis Th-1 and Th-2 activation
TLR express in Endothelium Fibroblast Vascular smooth muscle Memory T cell Mast cell Dendritic cell By nature a pro-inflammatory signaling receptors
RhoA-GTP Rho/Rock pathway Smooth muscle cell differentiation gene expresion Rho A– small GTPase( 20kDa) Ca+2 sensitize forcce RLC phosphorylation
GPCR GPCR PLC PIP2 Rock Rock IP3 Gq DAG Tyrosine kinase Src, FAK… SR Rock Ca+2 Dissociation of MLCK activity PKC RhoA-GDP RhoA-GTP RhoGDI AA Rock Rock Gq GPCR MyosinIIRLC20 G12/13 MLCP Ca-CaM MYPT1 P +PPIC MLCP inhibited MyosinIIRLC20 P Gene transcription
Asthmatic epithelial cells Reduced demosomal contact which may cause epithelial damage More susceptable to apoptosis Slower repair response Increase in number of mucus- containing cells Increase in the size of submucosal gland
Airway epithelial cell recognition of microorganisms is considered as an protective response in innate immunity • Air way epithelial cells secret large arrays of molecules that involves in inflammatory • Secretion causes chemotract and innate immunity
Damaged epithelial cells • TGF- release which promote the transformation of • fibroblast to myofibroblast Synthesis of cytokines, remodeling of airway, chronic inflammatipn release of Endothelin-1: smooth muscle mitogen) ectaxin : chemotractant for eosinophil vascular endothelial growth factor : promote growth of new blood vessel
Communication of asthmatic epithelium and mesenchyme by growth factors ►Susceptable to damage and repair leads to chronic inflammatory cycles
Stimuli and signals mediating synthesis of immune modulators in smooth muscle cells stimuli IL-1 IL-5 IL-13 TNF ERK1/2 JNK JAK IKK Signal transduction P38 MAPK NFB STAT Cytokines IL-1 IL-5 IL-6 IL-11 GM-CSF Other modulators Cox-2 IFN- Stem cell factor TNF VEGF Chemokines Eotaxin IL- MCA1,2,3 MIP1 RANTES
Cytokine Chemokine Growth factor T-cell Eosinophil Mast cell
IL-13 transgenic mouse Normal mouse Airway remodling in mouse overexpressin IL-13
Increased deposition of extracellular matrix( ECM) ECM: secret polysaccharides and proteins i.e. proteoglycan → modify binding of cytokines to cell surface receptors →storage of soluble factors in matrix In asthma patients → increase numbers cells in synthesize matrix protein → difference in degradation of existing proteins → more collegen I, III, V in submucosa membrane increase level of tenacin, lumican, biglycan, verican….. MMP( Metalopreteinase) : degrade ECM release cryptic information from ECM to liberate bioactive fragments lower MMP2, MMP-3 activity higher MMP-9 activity higher TMP-1( tissue-specific inhibitors of metalopreteinaase)
Comparative study of Airway smooth muscle remodeling Gastric fluid acid ??? Ovalbumin ???? Other excerbating factors ????
1st year 8 weeks control 8 weeks Gastric fluid aspiration Trachea Lung function assesment Animal sacrifice Provocative test 8 weeks Immunohistochemistry of tracheal and lung tissue Matrix protein profile assesment OVA sensitize Serum collection and BAL collection Evaluation of pro-inflammatory cytokines and immunoglobulin MMP profile assesment
In vitro study of airway smooth muscle remodeling Treatment of gastric fluid acid, or Rho kinase inhibitor Primary culture of air way smooth muscle cells Cell surface protein Elisa assay MMP Assay Rho/Rho kinase activity assesment Apoptotic assay Migration assay
Extracellular matrix protein Chemotaxis activation Rat gastric fluid acid Hyperplasia migration Smooth muscle cell apoptosis