Download
1 / 63
640 likes | 778 Views
Medical Device Evaluation and Validation. Harold Alexander, Ph.D. Orthogen Corporation Springfield, NJ Halexander@orthogencorp.com. Introduction. Vast experiment underway 20 million people (1 in 14) in USA with implants Vast experiment with no data collection

E N D
Medical Device Evaluation and Validation Harold Alexander, Ph.D. Orthogen Corporation Springfield, NJ Halexander@orthogencorp.com
Introduction • Vast experiment underway • 20 million people (1 in 14) in USA with implants • Vast experiment with no data collection • With exception of occasional reports of clinical failures, little is know about biomaterials performance in the human clinical environment
No good, long term, systematic studies have been performed. • A registration system for implants and biomaterials? • When we consider issues of long-term survival of biomaterials in vivo, the lack of attention to epidemiology and physiology are key issues. Researchers must become more careful and observant of clinical performance. • A national database of clinical data is essential to this effort.
Materials Selection • Currently used materials are survivors of a trial and error process. • Materials borrowed from other industries • Cost prohibitive for development of unique biomaterials. • Industry, until recently, could not afford it • Less than optimal materials.
Unique Biomaterials? • Few new candidate materials waiting for adoption. • Medical-legal environment argues for unique biomaterials. • Tissue Engineering Efforts.
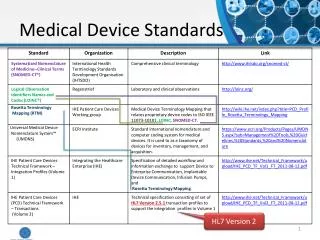
Biologic Safety • ASTM F 981-87: Standard Practice for Assessment of Compatibility of Biomaterials • Tripartite Biocompatibility Guidance
Animal Functional Tests • In use simulation • Safety • Efficacy
Clinical Studies • Initial Studies, Short term safety • Clinical Protocol • Prospective, Controlled, Randomized • Multi-Center • Assess mid-term safety and efficacy • Marketing Application • Long term follow-up (post-market?)
Regulatory Primer • Device Law passed in 1976. • Methods to introduce new medical devices: • Investigational Device Exemption Application • Clinical trials • Premarket Approval Application. or • 510(k), substantial equivalency application.
Device Retrieval & Analysis (DRA) • Devices that fail in service are not routinely analyzed • Studies address device in absence of clinical data • Clinical studies focus on patient, ignoring device issues
DRA (Continued) • Knowledge from small, non-random sampling. • Need to study 10% of devices that fail. • Greater need to study 90% that do not fail!
Sample Cases • Manufacturing flaw • Excess blast material on a total knee replacement • Manufacturing flaw • large grain size in ceramic ball • Design flaw • Inadequate stress analysis of hip acetabular component • Manufacturing procedure flaw • Residual machine oil on hip acetabular component
DePuy LCS Knee • Manufacturing flaw • Excess blast material on a total knee replacement
Feldmuhle Ceramic Hip Ball • Manufacturing flaw • large grain size in ceramic ball
DePuy ACS Cup • Design flaw • Inadequate stress analysis of hip acetabular component
Sulzer Acetabular Component • Manufacturing procedure flaw • Residual machine oil on hip acetabular component
Ethical Concerns • Professional Status • Professional status creates special obligations to use one's specialized skill and knowledge to promote significant social values (e.g., health), to protect the interests of those (clients) who will use the products you design and build, and to be a loyal employee.
Professional Obligations • Professional obligations take many forms, including: • a. using care in design to make sure that devices are safe and effective (promoting health); • b. protecting consumer autonomy, the right to make informed choices about health problems; • c. promoting and protecting your employer's legitimate interests.
One of the vexing problems of professional ethics is that these areas of obligation are often in conflict, requiring ethical judgment about how best to balance these conflicting demands!
Sample cases • Bjork-Shiley artificial heart valve • Silicone Gel-filled breast implants • Pedicle Screw Spinal Fixation • DePuy ACS Acetabular Cup • Effect of Radiation Sterilization • Guidant Heart Defibrillator
Bjork-Shiley artificial heart valve • unexpected defects in the welding of the valve led to catastrophic failure in a small percentage of them; • about 2/3 of those experiencing valve failure will die; • Shiley failed to warn patients, who were then unable to make informed decisions about their possibly defective heart valves; • there is evidence of poor manufacturing techniques at Shiley; what were the obligations of those who were aware of them?;
Bjork-Shiley Valve (continued) • Who should inform patients of possible defects? The patient's physician? The manufacturer? The Food and Drug Administration • What should patients be told? Only scientifically valid and reliable research? Reports of poor manufacturing techniques? • What if bioengineers are aware of a defective design or poor manufacturing techniques but the company is not responsive the their concerns? • What policies should guide these issues concerning medical devices and the patients who receive them?
Silicone Gel-filled Breast Implants • First introduced in 1964. • Grandfathered as pre-1976 device - 510(k) allowance. • FDA advisory panel recommended IDE - PMA study in 1978 because of safety concerns (bleed, rupture, inflammation, capsular contracture, calcification, autoimmune disease). • Plastic surgery lobby with aid of Ronald and Nancy Reagen prevented clinical review! • Law suits started in 1984. Reached level of 10s of thousands of cases by early 1990s.
Breast Implant (continued) • Device removed from market because of safety concerns in 1992. • To escape enormous legal liability, Dow Corning declared Chapter 11 bankruptcy in 1995. • Law suits against Baxter, Bristol Meyer Squibb, 3M and Dow Corning are now settling with an estimated total cost of 5 billion dollars. • Who is at fault? manufacturers, their employees, FDA, plaintiff lawyers, surgeons?