Download
1 / 38
0 likes | 11 Views
hope my presentation will be welcomed from you

E N D
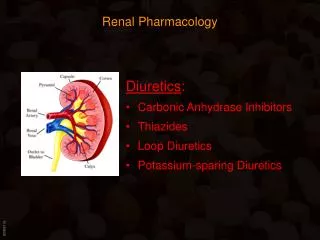
RENALPHARMACOLOGY Dr. Amany Tawfik Elfakhrany Lecturer of Clinical Pharmacology Faculty of Medicine – Menoufia University
Objectives:(ILOs) • Classifydiureticsaccordingtotheirmodeandsiteof action • Nametheprototypedrugandsomeotherdrugsineach class • Explainthemechanismofactionofeachclassandtheir pharmacologicaleffect. • Listtheclinicalusesandthemainadverseeffectofeach class • listtheelectrolyteimbalancethatmostcommonly occursasaresultofdiuretictherapy
Definition of Diuretics • Diuretics are drugswhich causea netloss of sodiumandwater from the body by an action on the kidney. Their primary effect is to decrease the reabsorption of sodium and chloride from the filtrate, increased water loss being secondary to the • increasedexcretionofthesalt. • Classificationofdiuretics: • Accordingtotheirsiteofaction: • 1. Extrarenaldiuretics(outsidethekidney) • InhibitingADHreleasee.g.water,hypotonicsolutionsðanol. • BlockingADHactione.g.lithium,demeclocycline. • Increasingthecardiacoutputandincreasingrenalbloodflowe.g.digitalis, dobutamine,theophyllineanddopamineincasesofHF. • 2Renal diuretics Classification of Diuretics
Site1: (proximalrenaltubule): It is a site of action of osmotic diuretics, secondary site of action of loop diuretics,oneofthesitesofactionofCarbonic Anhydrase(CA)inhibitors. • Site 2: thicksegmentoftheascendinglimbofloopof Henle):Itisthesiteofactionofloopdiuretics. • Site3: earlysegmentofdistalconvolutedtubuleor corticaldilutingsegment): It isthe siteof action of thiazide. • Site4:(distalpartofdistalconvolutedtubulesand collectingduct):ThesiteofactionofK+sparing diureticsandCAinhibitors.
Accordingtotheirnatriureticcapacityinto : Highefficacy:cause15-25%offilteredsodiumtobeexcreted. They remain effective at glomerular filtration rates (GFR) below 10 ml/min (normal127ml/min)e.g.loopdiuretics (highceiling diuretics(. Moderateefficacy:cause5-10%offilteredsodiumtobeexcreted. Theyare ineffective oncethe glomerular filtration rate hasfallen below20ml/mine.g.(thiazidesandtherelateddrugs( Lowefficacy:cause5%offilteredsodiumtobeexcreted.Usually combinedwith moreefficacious diuretics e.g. triamterene, amilorideandK+sparingdiuretics.
Thiazide diuretics Mechanismofaction: They actmainlyontheearlysegment ofthedistaltubule (cortical dilutingsegment),where they inhibitNaCl reabsorption. They decrease sodium reabsorption by inhibiting the Na+/Cl− cotransporter.ExcretionofCl-,Na+and accompanyingH2Ois increased. TheincreasedNa+loadinthedistaltubulestimulates Na+ exchangewith K+,increasing itsexcretionandcausing hypokalaemiaand metabolicalkalosis.
Pharmacologicalactions: • Renalactions: • TheyincreaserenalexcretionofNa+,Cl-,K+,HCO3-andwater. • TheyincreaseCa2+reabsorptionindistaltubulesresultingindecreaseCa2+excretion. • Theydecreaseuricacidexcretionduetocompetitioninhibitionofthetubulartransportof organicacids. • Theyincreasetheurinaryoutflowofmagnesium. • Theydecreaseglomerularfiltrationrateduetodecreaserenalbloodflowthrougha directactiononrenalvasculature. • Theyincreasetherenalexcretionofbromideandiodide. • Paradoxicalantidiureticeffectindiabetesinsipidus: • Especiallythenephrogenictype(ADH-resistanttype),theyreduce polyureaand polydipsiabythefollowingpossiblemechanisms:- • Thiazidescausemildsodiumand volumedepletionbyinhibitingNa+andwater reabsorption in proximal part of DCTwith increases of, compensatory, sodium and water reabsorptioninproximaltubule.
Thiazides cause increased Na+load passing to the distal part of distal tubule andcollectingtubulesasacompensatorymechanism,Na+reabsorptionis increasedinthesesegmentswithsubsequentincreaseofwaterreabsorption. • Thiazides causedecreasedglomerular filtration rateasaresult ofreduction ofrenalbloodflow. • ThiazidesmayincreasethesensitivityofADHreceptorsintherenaltubules. • Antihypertensiveeffect: • Thiazides are the preferred class of diuretics as antihypertensive drugs when renalfunctionisnormalthrough:- • Thereductioninplasmavolumeandstrokevolumeassociatedwitha diuresisdecreasescardiacoutputand,consequentlyBP. • Mobilesodiumand waterfromarteriolar wallthus, the diameterof the lumen oftheblood vesselsincreasesandlessresistancetotheflowofblood throughthevessels.
ThiazidescausealterationinNa+,K+, Ca2+andMg2+intracellular concentrations whichmaydecrease vascularresponsetopressor substancesandincreasevascular responsetodepressorsubstances. • Thiazidescausedirectrelaxationof vascularsmoothmuscle.
Therapeuticuses • Treatment of edemaand ascites due to mild to moderate CHF,chronic renalandhepaticdiseases, nephroticsyndrome,toxaemiaofpregnancyand premenstrualtension. • Essential hypertensionas aninitial therapy or in combination with β- blockers orvasodilators. • Treatmentofnephrogenicdiabetesinsipidus. • Treatmentofhypercalciuriaassociatedwithrecurrentrenalcalciumstones. • Treatmentofbromideoriodideintoxication. • Thiazideshaveaprotective effect inpatientsatriskforosteoporosisand longbonefracture.
Adverseeffects: • Hypokalaemiaandmetaboilcalkalosis; • Hypomagnesemiamayleadlocardiacarrhythmias. • Theplasmauricacidiselevated(hyperurecemia)andmayprecipitateacute goutyarthritis. • Hyperglycemiaduetoinhibitionofinsulinreleaseand/orblockadeoftheperipheralutilizationofglucose. • Transient increase in total cholesterol and triglycerides because thiazide induces insulin resistancewhichleads to basal hyperinsulinemia,which in turn, leadsto increasesynthesisandreleaseoftriglycerides. • Hypercalcaemia
Hyponatraemia:Thisisunusualbutpotentiallyserioussideeffects. • Hypersensitivityreactions(skinrash,fever,blooddyscrasia, pancreatitis, acutepulmonaryedema,dermatitis,cholestatic jaundice, thrombocytopeniaandhemolyticanaemia)arerelatedto sulphonamidemoietyandthereiscrosssensitivitywithother sulphonamide. • Thiazidemayprecipitateencephalopathyinhepaticinsufficiencydue toexcessivedepletionoffluidsandelectrolytes(especiallyK+.( • Anaemia,gastricirritation,maleimpotence,dizziness,vertigo, paraesthesia,andfatiguability. • :Contraindications • Diabetesmellitus, gout, decompensatedliver cirrhosis, hypersensitivity to thiazide,atherosclerosis,andrenalimpairment.
Drug-interaction: • Thiazidesmayprecipitatedigitalistoxicityinpatientsreceivingdigitalis. • Thiazideadministeredwithcorticosteroids;severehypo-kalaemiamay occur. • Thiazides increase plasma lithium concentration if combined with lithium. • Thiazides can reduce the effectonbloodsugarproducedby antidiabeticdrugs. • Theconcurrentuseofthiazideandtrimethoprimand sulphamethoxazoleinelderlypatientswithCHFproducesariskof thrombocytopeniawithpurpura. • Thiazidesmayincreasetheskeletalmusclerelaxantactivityof tubocurarineandgallamineduetothiazide-inducedpotassium deficiency.
Loop or high ceiling diuretics • Thesediureticsshareincommonthefollowingproperties: • Highpotency:Theyare themostpowerfulofalldiuretics causing15-25%ofsodiuminthefiltratetobeexcreted. • Shortdurationofaction2-4hrs. • Promptonsetofaction0.5-1 hrafteroraladministrationand 5-10min,followingIVinjection. • EffectiveatlowGFRevenbelow10ml/min. • They include: • Furosemide,bumetanide,andethacrynicacid.Furosemideand bumetanidearebothsulphonamidebutethacrynicacidisa phenoxyaceticacid derivatives.
Mechanismofaction: • They inhibit NaClreabsorption in the thick ascending loop of Henle. Theyactonthe luminal membranewhere theyinhibit the cotransport ofNa+/K+/2Cl. • TheymayalsoinhibitNaClreabsorptionintheproximaltubules. • They haveavenodilator actiondirectlyand/orindirectlythrough stimulating cyclooxygenase activity resulting in increased synthesis of vasodilatorprostaglandinsPGE2andPGI2.Theseprostaglandins maycontributeintherenalhaemodynamicchangesproducedby these drugs, increase glomerular filtration and also increase water and sodiumexcretion. • Pharmacologicalactions: • Theyare potentdiureticsincreasingNa+andCl-excretioninurine alongwithanequiosmoticamountofwater. • TheyenhancetheexcretionofbothCa2+andMg2+.
Theyenhancek+secretion at distal tubulesdueto increaseNa+load at this segmentwhichstimulate Na+reabsorptionin exchangewith K+ atthissegment. • They increase renal blood flow and cause redistribution of bloodflow withinrenalcortex. • Theyareweakinhibitorsofcarbonicanhydraseenzyme. • TheyhaveimmediatevenodilatoractionafterIVadministration. • Theydecreaseurinaryexcretionofuricacid. • Hyperglycemiaduetodecreasereleaseofinsulinlessthan thiazide.
Therapeutic uses: • Acutepulmonaryedema:Intravenousfurosemideorbumetanidedecreases intravascular volume and preload, so improvingpulmonarycongestion • Edematousconditionsduetochronicheartfailure,hepaticcirrhosis complicated by ascites andnephroticsyndrome. • Inhypertension, especiallyinindividualswithdiminishedrenal function. • Hypertensiveemergenciesandcerebraledema. • Inacute renal failure, they are used early to increase the rate of urine flow and enhance K+ excretion to convert oliguricrenal failure to non-oliguricfailure. • Treatmentof hypercalcaemia,theyblockcalciumreabsorption andhence they increase calcium excretion.
Adverseeffects: • Hypovolaemiaandhypotension. • Hypokalaemia andmetabolicalkalosisduetohydrogenion excretion. • Hypomagnesemiaand hypocalcemia. • Hyperuricemia. • Hyperglycemia (hypokalemialeadstodecreasedinsulin( • secretion resulting in hyperglycemia). • 6. Dose-relatedototoxicityintheformofdeafness,mayormay notbereversible. • 7. Allergy and cross allergy between furosemide and sulfonamide. • .
Drug-interaction: • Furosemidepotentiates the nephrotoxicityandototoxicity of aminoglycosides andcephalosporins. • Theycompetewithwarfarinandclofibrateforplasmaproteinbindingsites. • Theyprecipitatedigitalistoxicityinpatientsreceivingdigitalis. • Loopdiureticsadministeredwithcorticosteroids,severehypokalaemiamay occur. • NSAIDse.g.,indomethacinandaspirinreducethenatriureticand • diureticeffectsoffurosemidebecausetheseeffectsmaybemediated throughfurosemideinducedincreaseinsynthesisofPGE2andPGI2. • Condraindications: • Decompensatedlivercirrhosis,diabetesmellitus,andgout.
Potassium sparing diuretics • Thepotassiumsparingdiureticsfallintotwogroups: • Spironolactone:Thisinhibitstheactionofaldosterone. • Amilorideandtriamterene:Whichblockluminalsodiumchannels. • Alloftheseagentsexertaweakdiureticeffectanddecreasetheexcretion ofpotassiumandhydrogenion.
Spironolactone Spironolactone • Mechanismofaction: • Itactsbycompetitivelybindingtocytoplasmic receptorsandpreventing subsequentcellulareventsthatregulateK+andH+secretionandNa+ reabsoption.Theresultis anincreasetheexcretion of Na+(Cl-andwater) andadecreaseintheK+secretion. • Activeonlywhenendogenousaldosteroneispresent.
Therapeuticuses • Diseasecharacterizedbyexcessivealdosteronesecretionaslivercirrhosis, congestiveheartfailure • Diagnosisandtreatment ofprimaryhyperaldosteronism • Treatmentofhypertensionandrefractoryedema,generallyincombination withthiazidesorloopdiuretics. • Hypokalaemiaoralongwithdrugsthatcauseite.g.looporthiazidediuretics. • Treatmentoffemalehirsutism, and acne. • Adverseeffects • HyperkalaemiaandhyperchloremicmetabolicacidosisduetodecreaseK+ andH+secretion. • Nausea, abdominalpain,pepticulcer,rash,drowsinessandmental confusion. Antiandrogenic effects (spironolactone binds to androgen receptorsproducinganantiandrogeniceffect,whileleaving estrogen unopposed) which can result in gynaecomastia, testicular atrophyand impotence in males. • Maycauseuricacidretention. • .
Drug-interaction: 1- Used in combination with amiloride, triamterene, angiotensin converting enzyme inhibitors or K+ supplements cause hyperkalaemia. 2- It antagonizes carbenoxolone effect in peptic ulcer. Contraindications: 1- Hyperkalemia. 2- Patients with renal failure because of the tendency to develop hyperkalemia
Amiloride and triamterene • Amilorideandtriamterenebindtoandblocktheepithelial sodiumchannels(ENaC)and thereby decrease absorption of Na+ and excretion of K+ in the cortical collecting tubule, independent of the presenceofmineralocorticoids. • They inhibit Na+/H+exchange at DCT and collecting tubules by a direct action on tubular transport, and thus inhibit H+excretion, resulting in some degree of alkalinization of the urine whichis lessmarked with amiloride. • They promote theexcretionofuric acidi.e. milduricosuric.
Therapeuticuses: • Treatmentofcongestiveheartfailure,hypertension,cirrhosisandedema duetosecondaryhyperaldosteronism.. • Adverseeffects: • Hyperkalaemia. • Nauseaandvomiting. • Triamtereneisaweakfolicacidantagonistandcanleadto megaloblastic anemia ,especially in cirrhotic persons. • Contraindications:asspironolactone. • Drug-interaction: • Combinationwithspironolactoneorangiotensin convertingenzyme inhibitorscausesseverehyperkalaemia. • Triamtereneusedincombinationwithindomethacinhasproduced acuterenalfailure.
OSMOTIC DIURETICS • Theyaresmallmolecularweightcompoundswhichhavethefollowing features: • Theyarefilteredfreelythroughtheglomerulus. • Theyareincompletelyreabsorbedornotreabsorbedatallbythe nephron. • Theyarepharmacologicallyinertandlargerlyexcretedwithout metabolicchanges. • Mechanismofaction: • Mannitol iseasilyfilteredattheglomerulusbutpoorly reabsorbed. It increases the osmotic pressure of the glomerular filtrate, which inhibits the reabsorption of water and electrolytes and increases urine output.
Therapeutic uses: • Cerebraledema. • Acutecongestiveglaucoma. • Prophylaxisof acuterenalfailureresultingfromphysical traumaor surgery • Adverse effects: • Transientexpansionofplasmavolumeandhyponatraemia,thiscould cause cardiacfailureorpulmonary edema. • Headache,nausea,andvomiting • .
Contraindications • Severlyimpairedrenalfunclion. • Activeintracranialbleeding. • Markeddehydration,pulmonarycongestion. • pulmonaryedemaandheart failure.
Carbonic anhydrase inhibitors Mechanismofaction: Carbonic anhydrase (CA) is an enzyme predominately foundin theproximalconvoluted tubuleof the nephron. Itcatalysesthedehydrationof H2CO3to C02at the luminal membrane and the rehydration of C02to H2CO3 inthe cytoplasm . CA inhibitors causereversible inhibitionof the carbonic anhydrase enzyme leading toreduced sodium and bicarbonatereabsorption and, therefore,increased excretionofsodium, bicarbonate, and water
Therapeuticuses: CAinhibitorsarerarelyusedasdiureticsasitisweakand self-limiting. Glaucoma. Alkalinizationofurine. MountainSickness. Epilepsy.
Adverseeffects : Metabolic acidosisdueto reduction in bicarbonatestores. Drowsiness and paraesthesia occurfollowinglarge dose. Allergyandcross allergywithsulfonamide. Kidneystonesduetourinealkalinitythatdecreasesthesolubilityofcalcium (Ca2+) salts. Precipitatehepatic encephalopathy in hepatic cirrhosis.
: Contraindications • Hepaticcirrhosisbecausetheydecreaserenalexcretionofammonia. • Pregnancy. • Acuterenalfailurebecause they cause acidosis. • Preparations • Acetazolamide:
ACKNOWLEDGEMENTS • I oblige to pay my deep gratitude for the patience of hearing from all my medical students. Dear Students All Questions are Welcomed Amany.elfakharany@med.menofia.edu.eg