Download
1 / 75
770 likes | 833 Views
Learn about visual perception, its process, and components in the CNS for decision making. Explore visual cognition, memory, scanning, and attention. Discover pathways and streams for cognitive processing. Enhance your understanding of visual processing.

E N D
Visual perceptualDysfunctions and Assessment کارگاه تخصصی ادراک دیداری و شناخت دکتر مهدی علیزاده تابستان1396
What is visual perception ? • The ability to use vision to adapt to the environment which requires the integration of vision within the CNS to turn the raw data supplied by the retina into cognitive concepts of the perception of space and objects that can be manipulated and used for decision making . • The process by which this occurs is known as visual perception .
How it works ? • It occurs through visual processes
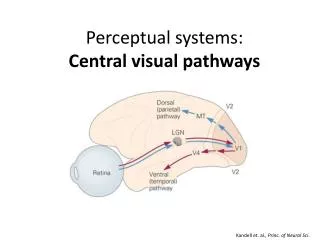
Visual processing within the CNS RETINA : RODS AND CONES , BIPOLAR CELLS , GANGLION CELLS FROM OPTIC CHAISMA FROM OPTIC TRACT TO LATERAL GENICULATE NUCLEUS VIA GENICULO CALCARINE TRACTS TO VISUAL CORTEX
The visual cortex is the part of the cerebral cortex responsible for processing visual information, and is located in the occipital lobe. • The term visual cortex refers to the primary visual cortex (also known as striate cortex or V1) and extra striate visual cortical areas such as V2, V3, V4, and V5. • http://wiki.bethanycrane.com/introducingtheeye
Dorsal Stream Ventral stream Primary cortex transmits information to two primary pathways – The dorsal stream and The ventral stream. Visual input travels from the visual cortex through parietal and posterior temporal circuitry to the prefrontal lobe to complete cortical visual processing The ventral stream is responsible for form recognition, object representation, conscious perception of environment and is associated with Long term memory storage The dorsal stream is associated with motion, the position of objects in the world, engagement with the environment and control of the eyes/arms (especially when visual information is used to guide saccades).
COMPONENTS OF VISUAL PERCEPTUAL PROCESSING • visual perceptual processing can be defined in a hierarchical model. • It consist of process of visual cognition , visual memory, pattern recognition, visual scanning and visual attention .
The highest order visual perceptual process in the hierarchy is visual cognition. • These perceptual processes are supported by three basic visual function that forms the foundation of the hierarchy : OculomotorControl,Visual Fields ,Visual Acuity • Visual cognition : It is a ability to manipulate and integrate visual inputs with other sensory information to gain knowledge, solve problems, formulate plans , and make decisions.( For the complete cognitive processing)
For example • Adult standing at a distance.
Visual memory • Visual memory : visual cognition cannot occur without the presence of visual memory. • The mental manipulation of visual stimuli requires the ability to create and retain a picture of the object in the mind’s eye while the visual analysis is being completed.
Pattern Recognition • Before the visual image can be stored in memory , and individual must recognize the pattern making up the image . • Pattern recognition, which sub-serves visual memory in the hierarchy , it involves identifying the object from the surroundings. • A salient feature is one that distinguishes a particular object from another .
For example • E F • T L • Green apple and red apple • To see its general shape, contour and features like color, shading, and texture .
Pattern recognition can not be accomplished without the next process in the hierarchy : • visual scanning : It is accomplished through the use of saccadic eye movements . A saccade is a movement of the eye towards an object of interest in the environment .
Visual attention • Visual scanning is actually a product of visual attention . • Visual search occurs on two levels : • An automatic or reflexive level- (controlled by brain stem)Any novel object moving or sudden appearing in the peripheral visual field, such as a flash of light. This response serves to protect an individual from unexpected intrusions in the environment. • A voluntary level- (directed by the cortex), is complete for the explicit purpose of gathering information .
Visual attention • Visual attention is a critical prerequisite for visual cognitive processing • If and how a person attends to an object or information determines if and how that visual input is analyzed by the CNS, which becomes the basis for decision making . • People who do not attend to visual information do not initiate a search for visual information , do not complete pattern recognition , do not lay down a visual memory and cannot use this visual input for decision making .
Engagement of visual attention and the other higher level processes in the hierarchy cannot occur unless the CNS is receiving clear, concise visual information from the environment . • Visual input is provided through the visual functions of oculomotor control, visual fields and visual acuity.
Oculomotor control : It enables eye movement to be completed quickly and accurately and ensures perceptual stability . • Visual fields : Which lets the brain know what's going on in the environment . • Visual acuity : Ensures that the visual information sent to brain is accurate.
Disorders of visual perception are found in : • Stroke • Intracranial compressing masses • Neurosurgical procedures • Demyelinating disorders • Neurodevelopmental conditions (eg, autism) • Neurodegenerative disease • Schizophrenia and depression.
Purpose of the assessment • To identify the limitation in activity or occupation. • To link that limitation to presence of a visual impairment • To develop an appropriate intervention plan based on the results of the assessment .
Occupational therapy assessment of specific visual –perceptual impairments • Visual acuity : It is commonly measured by Snellen fraction. • Normally :( 20/20) it means that a person can see the letter that a person with normal vision can see at 20 feet. The common Defects of visual acuity are : • Myopia(nearsightedness), • Hyperopia(farsightedness)
3. Astigmatism- It is an optical defect in which vision is blurred due to the inability of the optics of the eye to focus a point object into a sharp focused image on the retina. . Assessed by : LeaNumbers low vision test chart and warren text card
Visual field • Visual field defect is caused due to damage to the receptor cells in the retina optic pathway that relays retinal information to CNS for processing results in a visual field deficits . • Conditions occuring in VFD are : • Heminanopsia: There has been loss of vision in one half of the visual fields in the eyes. • Homonymous : it means deficit is same in both the eyes. • The assessment of the VF is know as perimetry test these ranges from simple confrontation test to more precise imaging of a scanning laser opthalmoscope (SLO).
Screening of visual field deficits • Confrontation testing • Equipments: eye patch or patches • Set up : patient seated directly opposite to examiner, approx 20 inches eye to eye . • Background behind examiner should be dark and distraction free. • Procedure : patch the patient left eye and close or patch your own right eye • Instruct patient to look at your left eye and tell him or her you will be moving a target in from the side and the patient is to indicate when the target is first seen.
Move target in from all angles • Compare the patient response with yours. • Position hands at 3 and 9 clock so that you can just see your fingers . Ask the patient how many fingers you are holding up . • A problem is indicated if the patient cannot see the target when you do or does not see both fingers simultaneously.
Visual skills for reading test provides an effective way to measure the interference of the VFD on reading performance. • Perimetry devices such as the Damato 30 – point multifixationcampimeter ( biVABA). http://www.sussexvision.co.uk/damato-fieldscreener-30-point-p-5638.html
Visual attention and scanning • Condition which occurs due to defect of VA and scanning are : • Hemi- inattention : Instead of initiating from left to right visual search pattern, clients with right hemisphere injuries often begin and confine search to right side . • Visual neglect : it is a combination of hemi- inattention and left visual field defect (VFD).clients with this condition show exaggerated inattention towards the left half of the visual space surrounding the body and often do not move the eye past midline towards the left or turn head towards the left side .
Unilateral neglect Hemispatial neglect, also called hemiagnosia, hemineglect, unilateral neglect, spatial neglect, unilateral visual inattention, hemi-inattentionor neglect syndrome is a neuropsychological condition in which, after damage to one hemisphere of the brain is sustained, a deficit in attention to and awareness of one side of space is observed. It is defined by the inability of a person to process and perceive stimuli on one side of the body or environment that is not due to a lack of sensation. Unsworth, C. A. (2007). Cognitive and Perceptual Dysfunction. In T. J. Schmitz & S. B. O’Sullivan (Eds.), Physical Rehabilitation (pp. 1149-1185). Philadelphia, F.A: Davis Company.
Spatial neglect may result from lesions of the dominant parietal, temporal, or frontal cortex. • There are different types of unilateral neglect:(Eskes & Butler, 2001) • Personal neglect • Peri-personal neglect • Extra-personal neglect
Assessment • Assessment of lower level visual functions ( visual acuity , oculomotor function and visual field). • Letter cancellation test • Trail making • Brain injury visual assessment battery for adults.(Other specific scales are to be discussed later on)
Scan board test • Described by warren • Consist of large 20 by 30 inch board with a series of 10 numbers displayed in an unstructured pattern . • The board is placed at the eye level and centered at the client’s midline . • The client is asked to scan the board • Point out all of the numbers that are seen. • The examiner records the pattern the client follows .
Comparision of search pattern : person with visual field defect vs hemi- inattention From Warren M:Brain injury visual Assessment battery
Occulomotor function deficit • Deficit in oculomotor control following brain injury generally results from either of two types of disruption • Specific cranial nerve • Disruption of central neural control of the extra ocular muscles affecting the coordination of eye movements .
Oculo motor function • The defects is associated with cranial nerve injury . • Oculomotor nerve (3): impaired vertical eye movements , lateral diplopia for near vision tasks, dilation of pupil and impaired accomodation , ptosis of eyelid. • Trochlear nerve (4) : impaired downward and lateral eye movements, vertical diplopia for near vision tasks • Abducence nerve (6) : impaired lateral eye movements, lateral diplopia for far vision tasks.
Assessment of oculomotor function • Ask the client about the expercience of diplopia : • Look for the diplopiadisappering when eye closed • Which side lateral or vertical • Far or near • The next part of the assessment is observing the client eye and eye movement for deficiencies • The eye are observed for asymmetries in pupil size , eyelid function and eye position as the client focuses on a distance object .
Look for ptosis • Tracking of the moving object : in figure of H or X pattern • Note the point of convergence ( normally approx 3 inches from the bridge of nose ). • Eye ball movement
Assessment of specific visual perceptual impairments • Visual object Agnosia: caused due to lesion to the right occipital lobe . In this the person is unable to recognize and identify an item using visual means. • Assessment is performed by asking the individual to identify five common objects by sight. • Color agnosia: Refers to inability to remember and recognize the specific colors for common objects in the environment. Also know as Central Achromatopsia • Assessment : present the client with two common objects that are accurately colored and two objects that are not accurately colored . Ask the patient to pick the object that are not accurately colored. • Color Anomia: refers to the client’s inability to name the color of the object. while the client understand the differences between the different colors of objects, they are unable to name the color of the object accurately .
Color anomia: ask the client to name the color of various objects in their environment . • Metamorphopsia : refers to visual distortion of objects, such as the physical properties of size and weight .Assessment includes presenting the client with various objects of different weights and sizes. • Prosopagnosia : refers to an inability to recognize and identify familiar faces caused due to lesion of the right posterior hemisphere . • Non standardized test : to identify the names of the people in photographs, with family members
Simultanognosia : refers to the inability to recognize and interpret a visual array as a whole and is caused by lesion to the right hemisphere of the brain . • The person is able to identify the individuals components of a visual scene , but are unable to recognize and interpret the gestalt of the scene . • Assessment : presenting the client a photograph of a detailed visual array .
Right – left discrimination : • It is the inability to identify the right and left sides of one’s own body or of that of the examiner . • The person with right and left discrimination cannot tell the therapist which is the right arm and which is the left . • It is caused due to lesion at the parietal lobe of either hemisphere • Testing : ask the person to point to body part on command, such as : right ear, left foot, right arm.
Visual-spatial perception Disorders • It refers to appreciate the spatial arrangement of one’s body, objects in relationship to oneself, and relationship between objects in space. • Figure-ground discrimination: it is a inability to visually disctinguish a figure from the backgroung in which it is embedded. • The patient cannot locate items in a pocketbook or drawer, locate buttons on a shirt. • It is caused due to parieto-occipital lesion of the right hemisphere and less frequently the left hemisphere commonly produce this disorder. • It can be assessed functionally in a variety of contexts . During a dressing activity, or by asking in the client to pick one utensil out of many utensils . • The Ayres Figure-ground Test( subtest of the southern California sensory integration tests)
Form discrimination • Form discrimination : It is inability to perceive or attend to subtle difference in form and shape . The patient is likely to confuse objects of similar shape or not to recognize an object placed in a unusual position. • It is caused due to lesion at the parieto-temporo-occipital region of the non-dominant lobe. Testing : A number of items similar in shape and different in size are gathered. The patient is asked to identify them. Visual agnosia must be ruled out first.
Spatial Relations • Spatial disorientation, is the inability to perceive the relationship of one object in space to another object, or to oneself. • It is caused due to lesion to the inferior parietal lobe • Testing : The patient may be unable to tell the time from a clock because of difficulty in perceiving the relative positions of the hands. Before testing unilateral neglect and hemianopsia should be ruled out . • Rivermead perceptual assessment battery(RPAB) • The Arnadottir OT-ADL Neurobehavioural Evaluation
Depth perception • In this the person experiences inaccurate judgment of direction, distance, and depth. • Caused due to lesion in the posterior right hemisphere in the superior visual association cortices. • To test the person is asked to fill a glass of water.
Position in space • It is inability to perceive and to interpret spatial concepts such as up, down, under, over, in, out, in front of, and behind. • The lesion is usually located in the non-dominant parietal lobe. • Testing : to test function, two objects are used, such as a shoe and a shoebox. The patient is asked to place the shoe in different position in relation to shoebox; for example, in the box, on top of box or next to box.
Vertical disorientation: it is the distorted perception of what is vertical . Caused due to lesion in the non-dominant parietal lobe. • Test by asking the person to place the cane vertically when it is placed horizontally . • Topographic disorientation: difficulty in understanding and remembering relationship of one location to another . • Caused due to lesion inferior parietal lobe or occipital association cortex and occipito temporal cortex. • Test by asking to describe or to draw a familiar root such as the block in which he lives .