Download
1 / 1
10 likes | 161 Views
Regional Variations and Trends in Antimicrobial Resistance Among E. faecalis (EF) and E. faecium (EFM) in the Global SENTRY Antimicrobial Surveillance Program (1997-2000). Percent susceptible/resistant by year (no. tested): a. Antimicrobial. 1997 (546). 1998 (508). 1999 (162). 2000 (455).

E N D
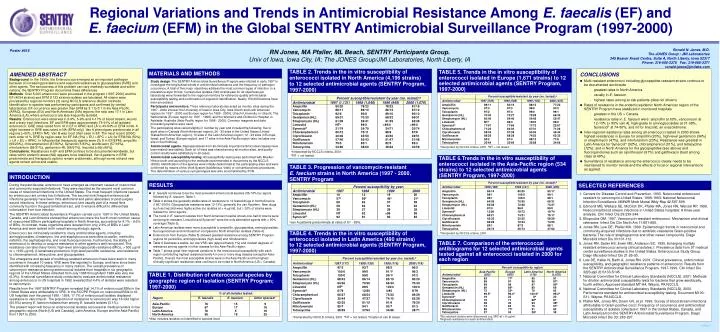
Regional Variations and Trends in Antimicrobial Resistance Among E. faecalis (EF) and E. faecium (EFM) in the Global SENTRY Antimicrobial Surveillance Program (1997-2000) Percent susceptible/resistant by year (no. tested):a Antimicrobial 1997 (546) 1998 (508) 1999 (162) 2000 (455) 1998 (188) 1999 (141) 2000 (205) 86/14 98/1 99/1 64/36 62/38 97/0 13/80 68/21 42/35 69/28 89/1 26/74 80/20 100/0 100/0 70/30 72/28 96/0 18/72 74/21 50/32 72/24 87/3 36/74 83/17 99/1 99/1 69/31 73/27 99/0 19/74 79/17 58/29 74/25 88/1 37/62 Percent susceptible/resistant by year (no. tested):a Antimicrobial 1997 (117) 1998 (139) 1999 (116) 2000 (118) Ampicillin Vancomycin Teicoplanin Gentamicin (HL) Streptomycin (HL) Linezolid Synercid Chloramphenicol Ciprofloxacin Gatifloxacin Nitrofurantoin Tetracycline 97/3 100/0 100/0 68/32 64/36 NTb 6/79 66/27 35/44 62/35 85/7 38/59 93/7 99/0 99/0 86/14 70/30 89/0 12/80 68/24 47/27 81/15 94/1 37/63 98/2 91/1c 99/1c 85/15 66/34 100/0 4/80 75/23 74/15 91/9 93/7 34/66 95/5 96/3 97/3 80/20 70/30 100/0 8/79 69/29 63/28 76/20 91/3 28/71 Region % of all isolates tested: E. faecalis E. faecium Other speciesa RN Jones, MA Pfaller, ML Beach, SENTRY Participants Group. Univ of Iowa, Iowa City, IA; The JONES Group/JMI Laboratories, North Liberty, IA Poster #515 Ronald N. Jones, M.D. The JONES Group / JMI Laboratories 345 Beaver Kreek Centre, Suite A, North Liberty, Iowa 52317 Phone: 319-665-3370 Fax: 319-665-3371 ronald-jones@jmilabs.com AMENDED ABSTRACT Background: In the 1990s, the Enterococcus emerged as an important pathogen because of increasing prevalence and acquired resistances to glycopeptides (GRE) and other agents. The seriousness of this problem can vary markedly worldwide and within nations; the SENTRY Program documents these differences. Methods: Over 8,000 enterococci were processed in the program (1997-2000) and the EF (4034 strains) and EFM (1123 strains) isolates are tabulated. All strains were processed by regional monitors (3) using NCCLS reference dilution methods. Identification to species was performed by participants and confirmed by central laboratories. EF occurrence was greater than EFM by 3:1 to 5:1 in the Asia-Pacific (APAC), European (EU) and North American (NA) regions; the ratio was 17:1 in Latin America (LA), where enterococci are less frequently isolated. Results: Enterococci were observed in 3-9%, 5-9% and 4-17% of blood stream, wound and urinary tract infections. EF and EFM were approximately 75-91% of all isolated enterococci. GRE rates varied from nil in EF in APAC and LA to 43-54% in EFM in NA. A slight increase in GRE was noted in NA (EFM only). Van A phenotypes predominate in all regions (>80%, EFM in NA). Van B was most often seen in EF. The most recent (2000) rank order of % GRE by region was: for EF-NA (3%) > EU > APC = LA; for EFM-NA (50%) > LA > EU > APAC. In NA potential therapeutic agents were (% S in EF/EFM): ampicillin (99/20%), chloramphenicol (87/90%), Synercid (1/83%), levofloxacin (57/18%), nitrofurantoin (98/31%), gentamicin-HL (68/61%), linezolid (>99/>99%). Conclusions: Resistances in EF and EFM continue to be documented worldwide, but rates within endemic areas (NA) appears to be stabilized. Van A patterns in EFM predominate and therapeutic options remain problematic, although some old and new agents remain active and usable. MATERIALS AND METHODS CONCLUSIONS • Multi-resistant enterococci including glycopeptide-resistant strains continue to be documented world-wide • greatest rates in North America • usually in E. faecium • highest rates among at-risk patients (data not shown) • Rates of resistance in the endemic/epidemic North American region of the SENTRY Program have stabilized in monitored hospitals • greatest in the US > Canada • resistance rates in E. faecium were: ampicillin at 80%, vancomycin at 12-13% (> 80% van A), high-grade to aminoglycosides at 31-38%, Synercid at 74-80%, and nil for linezolid, an oxazolidinone. • Inter-regional resistance rates among all enterococci tested in 2000 shows highest resistances in Europe for ampicillin (23%), high-level gentamicin (34%) or streptomycin (47%), and nitrofurantoin (23%). Resistance was greatest in Latin America for Synercid (92%), chloramphenicol (31%), and tetracycline (72%); and in North America for the glycopeptides (see above) and fluoroquinolones such as ciprofloxacin (61%) and gatifloxacin (best among class at 49%). • Surveillance of resistance among the enterococci clearly needs to be maintained to monitor trends and the effects of local or regional interventions as applied. TABLE 2. Trends in the in vitro susceptibility of enterococci isolated in North America (4,196 strains) to 12 selected antimicrobial agents (SENTRY Program, 1997-2000) TABLE 5. Trends in the in vitro susceptibility of enterococci isolated in Europe (1,671 strains) to 12 selected antimicrobial agents (SENTRY Program, 1997-2000) Study design. The SENTRY Antimicrobial Surveillance Program was initiated in early 1997 to investigate the longitudinal trends in antimicrobial resistance and the frequency of pathogen occurrence. A total of five major objectives address the most common types of infection, in a prevalence-style format. Consecutive isolates (540 strains/year for all objectives per laboratory) were forwarded to the regional monitors for reference-quality antimicrobial susceptibility testing and confirmation of organism identification. Nearly 150,000 bacteria have been processed. Participants and monitors. Three reference laboratories acted as monitor sites during the 1997 - 2000 interval: the University of Iowa in Iowa City, Iowa (North and Latin American regions for 1997 - 2000 and Europe region for 1999 - 2000); Utrecht University, in Utrecht, The Netherlands (Europe region for 1997 - 1998); and the Women’s and Children’s Hospital, in Adelaide, Australia (Asia-Pacific region for 1998 - 2000). Common reagents and data processing systems were used. The participating sites varied slightly in number by year and included the following: five to eight sites in Canada (North American region); 26 - 30 sites in the United States (United States/North American region), 10 sites in the Latin American region; 12 - 23 sites in Europe, Israel, and Turkey (Europe region); and 17 sites in the Asia-Pacific region (also includes one site in South Africa). Antimicrobial agents. Representatives from all clinically important antimicrobial classes have been tested (see tables). Each lot of trays was shared among all monitor sites, and quality control results were satisfactory in all cases. Antimicrobial susceptibility testing. All susceptibility testing was performed with Mueller-Hinton broth and according to the methods recommended in documents by the NCCLS (2000). Identification of the species were initially determined at the participating sites and were confirmed by means of the Vitek System (bioMerieux Vitek) or conventional test procedures. The determination of various van genotypes was also accomplished by PCR. Percent susceptible/resistant by year (no. tested):a Antimicrobial 1997 (1,131) 1998 (1,040) 1999 (949) 2000 (1,076) Ampicillin Vancomycin Teicoplanin Gentamicin (HL) Streptomycin (HL) Linezolid Synercid Chloramphenicol Ciprofloxacin Gatifloxacin Nitrofurantoin Tetracycline 89/11 97/3 97/2 70/30 60/40 NTb 17/67 71/23 58/35 68/26 93/2 35/64 84/16 97/3 97/3 73/27 54/46 98/0 17/66 64/30 57/38 68/28 87/4 32/66 88/12 99/0 99/0 72/28 54/46 100/0 17/73 67/31 50/35 74/25 88/12 32/68 77/22 97/2 99/1 66/34 53/47 99/0 22/67 71/26 45/44 62/33 77/8 34/66 Ampicillin Vancomycin Teicoplanin Gentamicin (HL) Streptomycin (HL) Linezolid Synercid Chloramphenicol Ciprofloxacin Gatifloxacin Nitrofurantoin Tetracycline 80/20 88/11 92/6 69/31 61/39 NTb 21/74 80/12 40/46 57/40 79/5 33/66 78/22 89/10 92/8 70/30 59/41 99/0 24/70 75/11 35/50 55/43 85/1 38/60 78/22 86/13 89/10 68/32 61/39 >99/0 24/71 88/9 43/50 51/47 82/5 38/62 81/19 87/12 90/10 69/31 62/38 >99/0 20/74 87/8 39/51 51/48 83/3 40/59 aInterpreted by NCCLS criteria, 2001. bNT = not tested. aInterpreted by NCCLS criteria, 2001. bNT = not tested. TABLE 6.Trends in the in vitro susceptibility of enterococci isolated in the Asia-Pacific region (534 strains) to 12 selected antimicrobial agents (SENTRY Program, 1997-2000) TABLE 3. Progression of vancomycin-resistant E. faecium strains in North America (1997 - 2000, SENTRY Program INTRODUCTION RESULTS SELECTED REFERENCES Percent susceptible/resistant by year (no. tested):a During the past decade, enterococci have emerged as important causes of nosocomial and community-acquired infections. They were reported as the second most common cause of nosocomial infections in the United States. The most frequent infections caused by enterococci are urinary tract infections. The second most frequent enterococcal infections generally have been intra-abdominal and pelvic abscesses or post-surgery wound infections. In these settings, enterococci are usually part of a mixed flora commonly found in the gastrointestinal tract, and it remains difficult to differentiate colonization from true infection. The SENTRY Antimicrobial Surveillance Program carried out in 1997 in the United States, Canada, and Latin America showed that enterococci were the fourth most common cause of nosocomial BSIs in participating hospitals in North America, accounting for 9.1% - 9.6% of BSIs. In contrast, these organisms were isolated from only 2.9% of BSIs in Latin America and were ranked ninth overall among etiologic agents. Enterococci are intrinsically resistant to many antimicrobial agents, including aminoglycosides, clindamycin, the anti-staphylococcal penicillins (oxacillin, methicillin, nafcillin), the cephalosporins, and most fluoroquinolones. Furthermore, the ability of enterococci to develop or acquire resistance to other agents is well recognized. This resistance can take many forms: high-level aminoglycoside resistance (MICs, > 500 g/ml or > 1000 g/ml), -lactamase production, high-level penicillin resistance, and resistance to chloramphenicol, tetracycline, and glycopeptides. The emergence and spread of multidrug-resistant enterococci have been seen in many countries in the past 10 years. VRE were first reported in Europe, and have since been identified with increasing frequency in many nations. The overall prevalence of vancomycin resistance among enterococcal isolates from hospitals in six geographic regions of the United States collected from July 1988 through April 1989 was very low (0.3%). A national surveillance study conducted to evaluate antimicrobial resistance among enterococci in US hospitals in 1992 revealed that 4.4% of isolates were resistant to vancomycin. Results from the 1997 SENTRY Program revealed that 14.1% of enterococcal BSIs in the United States were attributable to VRE. In the SCOPE Project on nosocomial BSIs in 49 US hospitals over the period 1995 - 1998, 17.7% of enterococcal isolates displayed resistance to vancomycin. The proportion of resistance to vancomycin was 16-fold higher (50.5%) among E. faecium isolates than among E. faecalis isolates (3.1%). The present report will focus on enterococcal isolates recovered at medical centers in four geographic regions (North [US and Canada], Latin America, Europe and the Asia-Pacific) from 1997 to 2000. Percent susceptibility by year: Antimicrobial Antimicrobial 1997 1998 1999 2000 Ampicillin Vancomycin Teicoplanin Gentamicin (HL) Streptomycin (HL) Linezolid Synercid Chloramphenicol Ciprofloxacin Gatifloxacin Nitrofurantoin Tetracycline • E. faecalis continues to be the most prevalent enterococcal species (56-76% by region) followed by E. faecium, Table 1. • Table 2 shows the generally stable rates of resistance to 12 tested drugs in North America (1997-2000). Glycopeptide resistance was 12-13%, generally the van A pattern. New drugs such as linezolid were highly active (no isolates at > 4 g/ml), but 20% of strains were resistant to other agents. • The trend in E. faecium isolates from North American hospital shows one-half of strains were vancomycin-resistant. Linezolid and Synercid were the only alternative agents with > 90% coverage (Table 3). • Latin American isolates were more susceptible to ampicillin, glycopeptides, aminoglycosides, fluoroquinolones and nitrofurantoin compared to North American isolates (Table 4). • Enterococci from Europe (Table 5) showed greatest resistance among SENTRY Program regions for penicillins, aminoglycosides (high-level) and nitrofurantoin. • Table 6 illustrates a stable, but low VRE rate (approximately 1%) and modest degrees of resistance among agents in other classes for the Asia-Pacific region. • Table 7 shows great inter-regional variations in the enterococcal susceptibility with each region contributing highest resistance levels for one or more drug classes (exception Asia-Pacific). Overall, the most susceptible strains were in the Asia-Pacific and the highest clinically significant resistance rates continue to be noted in North America (US > Canada). 1. Centers for Disease Control and Prevention. 1993. Nosocomial enterococci resistant to vancomycin-United States, 1989-1993: National Nosocomial Infection Surveillance. MMWR Morb Mortal Wkly Rep 42:597-599. 2. Edmond MB, Wallace SE, McClish DK, Pfaller MA, Jones RN, Wenzel RP. 1999. Nosocomial blood stream infections in United States hospitals: A three-year analysis. Clin Infect Dis 29:239-244. 3. Eliopoulos GM. 1997. Vancomycin-resistant enterococci. Mechanism and clinical relevance. Infect Dis Clin North Am 11:851-865. 4. Jones RN, Low DE, Pfaller MA. 1999. Epidemiologic trends in nosocomial and community-acquired infections due to antibiotic-resistance Gram-positive bacteria: The role of streptogramins and other newer compounds. Diagn Microbiol Infect Dis 33:101-112. 5. Jones RN, Sader HS, Erwin ME, Anderson SC. 1995. Emerging multiply resistant enterococci among clinical isolates. I. Prevalence data from 97 medical center surveillance studies in the United States. Enterococcus Study Group. Diagn Microbiol Infect Dis 21:85-93. 6. Low DE, Keller N, Barth A, Jones RN. 2001. Clinical prevalence, antimicrobial susceptibility, and geographic resistance patterns of enterococci: Results from the SENTRY Antimicrobial Surveillance Program, 1997-1999. Clin Infect Dis 32(Suppl 2):S133-S145. 7. National Committee for Clinical Laboratory Standards (NCCLS). 2001. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically, fourth edition: Approved standard M7-A4, Wayne, PA:NCCLS. 8. National Committee for Clinical Laboratory Standards (NCCLS). 2000. Performance standard for antimicrobial susceptibility testing. Document M100-S11, Wayne, PA:NCCLS. 9. Pfaller MA, Jones RN, Doern GV, et al. 1999. Survey of blood stream infections attributable to Gram-positive cocci: Frequency of occurrence and antimicrobial susceptibility of isolates collected in 1997 in the United States, Canada, and Latin America from the SENTRY Antimicrobial Surveillance Program. Diagn Microbiol Infect Dis 33: 283-297. Ampicillin Vancomycin Teicoplanin Gentamicin (HL) Streptomycin (HL) Linezolid Synercid 16 57a 68 58 28 NT 92 12 56a 63 62 27 92 91 19 46 a 57 61 29 >99 92 20 51a 59 63 38 99 83 avan A patterns predominate at rates of 81 - 89%. aInterpreted by NCCLS criteria, 2001. TABLE 4. Trends in the in vitro susceptibility of enterococci isolated in Latin America (490 strains) to 12 selected antimicrobial agents (SENTRY Program, 1997-2000) TABLE 7. Comparison of the enterococcal antibiograms for 12 selected antimicrobial agents tested against all enterococci isolated in 2000 for each region Percent susceptible by region: Antimicrobial Asia-Pacific (205) Europe (455) Latin America (118) North America (1,076) TABLE 1. Distribution of enterococcal species by geographic region of isolation (SENTRY Program; 1997-2000) Ampicillin Vancomycin Teicoplanin Gentamicin (HL) Streptomycin (HL) Linezolid Synercid Chloramphenicol Ciprofloxacin Gatifloxacin Nitrofurantoin Tetracycline 83 99 99 69 73 99.5a 19 79 58 74 88 37 77b 97 99 66b 53b 99.3a 22 71 45 62 77b 34 95 96 97 80 70 100.0a 8b 69b 63 76 91 28b 81 87b 90b 69 62 99.2a 20 87 39b 51b 83 39 Asia-Pacific Europe Latin America North America 76 67 76 56 15 17 5 19 9 16 19 25 aNo resistant strains were discovered e.g. MIC at 8 g/ml. bHighest resistance for each antimicrobial. aInterpreted by NCCLS criteria, 2001. bNT = not tested. cCluster of van B cases. aAlso includes isolates not identified to species level. A156-27