Download
1 / 23

E N D
1. Feezor Chief Roundtable
December 19, 2005 Total Parenteral Nutrition Robert J. Feezor, MD
University of Florida
Department of Surgery
2. Feezor Chief Roundtable
December 19, 2005
3. Feezor Chief Roundtable
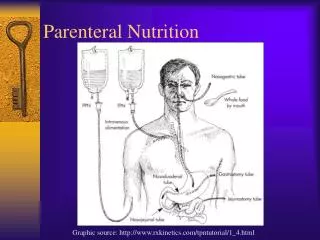
December 19, 2005 When to use TPN �If the gut works, use it!�
Assess patient�s nutritional status
History
Weight loss
Anorexia
Weakness
Inability to carry out normal functions
Disease process that interferes with intake
Physical
Muscle wasting
Loose skin
Edema of hypoproteinemia
Loss of body fat
4. Feezor Chief Roundtable
December 19, 2005 Nutritional assessment Indirect calorimetry
BEE (Harris-Benedict Equation)
Based on sex, weight, height, age
RQ = CO2 produced / O2 consumed
RQ = 1.0, pure CHO metabolism
RQ = 0.7, fat metabolism
RQ < 0.7, ketogenesis
Anthropometric measurements
Triceps skinfold measurements
IBW (males) = 48 kg + 2.7 kg for each inch over 5�0�
IBW (females) = 45.5 kg + 2.3 kg for each inch over 5�0�
5. Feezor Chief Roundtable
December 19, 2005 Nutritional assessment Functional studies of muscle
Biochemical measurements
Albumin (3.0 g/dL)
Prealbumin
Nitrogen balance
(Protein in (g)/ 6.25) � urinary urea
Protein breakdown
Immunologic function
6. Feezor Chief Roundtable
December 19, 2005 Malnutrition sequelae >10% weight loss:
Increased LOS
Increased incidence of nosocomial infections
Increased mortality
7-10 days of malnutrition:
Impaired complement and Ig production
Dysfunctional leukocyte chemotaxis, phagocytosis, oxidative burst
Poor tissue repair
Loss of muscle function: ventilator dependence
Up to 50% of inpatients are malnourished
7. Feezor Chief Roundtable
December 19, 2005 How to write TPN Specific Fuels
Theory
Practical Information
8. Feezor Chief Roundtable
December 19, 2005 Basic TPN Calculate MIVF rate:
4 � 2 � 1 rule
65 kg female
10 x 4 = 40
10 x 2 = 20
45 x 1 = 45
TOTAL = 105
1 L = 42 mL / hr
1.5 L = 63 mL / hr
2 L = 84 mL / hr Specific fuels:
Carbohydrate
Fats
Amino Acids
In general, amino acids are not included in kcal/kg figures:
�non-protein calories�
9. Feezor Chief Roundtable
December 19, 2005 Carbohydrate 3.4 kcal / g (anhydrous)
�Protein-sparing effect� by Gamble (1940)
As little as 100g glucose per 24h will decrease urinary urea production
Suppresses hepatic gluconeogenesis (avoids protein breakdown)
Exogenous glucose obviates need for amino acids as energy fuel
D5�NS @ 84 mL/hr = 100g dextrose per day
10. Feezor Chief Roundtable
December 19, 2005 Carbohydrate 3.4 kcal / kg (anhydrous)
�Protein-sparing effect� by Gamble (1940)
Excess glucose administration
Converted to fat in the liver: de novo lipogenesis
Immunosuppressant, increasing nosocominal infections
ICU control 1:
1548 patients all receiving 25 kcal/kg parenterally or enterally
Randomized to 180-200mg/dL or 80-110mg/dL
Mortality decreased by 42% in �tight glucose control� group
11. Feezor Chief Roundtable
December 19, 2005 Carbohydrate Start at 150g per day
What % Dextrose is this?
Why start here?
For a 70 kg person, this is 7.3 kcal/kg
(150 g x 3.4 kcal/g) / (70 kg)
Increase by 50 g per day
Watch PO4, which will decline
�Refeeding syndrome�
Check CS q6h
Adjust insulin in HAL to decrease SSI requirements
12. Feezor Chief Roundtable
December 19, 2005 Fat Optimally, 25% of nonprotein calories
Major source of fuel during starvation
During minor stress, CHO and fat utilization are indistinguishable in terms of Nitrogen balance
At some point during sepsis, fat utilization is impaired
Calorically dense (9 kcal/g)
13. Feezor Chief Roundtable
December 19, 2005 Fat Lipid accumulation in the liver overloads the Kupffer cells (hepatic macrophages)
Inhibits reticuloendothelial system
Excess lipid administration may increase PGE2 and thromboxane A2
Decreases the ability of the pulmonary hypoxic vasoconstriction
Worsens gas diffusion, oxygenation in ARDS
The phospholipid emulsifying portion of IL solution can interfere with lipoprotein lipase
Can increase serum triglycerides
Don�t administer IL in patients with TG>400
14. Feezor Chief Roundtable
December 19, 2005 Fat Start on 2nd day
Check TG on day#1
Why else do we wait?
250-500 mL per day
12 on / 12 off
Shands formula has 2 kcal / mL
500 mL = 42 mL/h x 12h
500 mL = 1000 kcal
(14.3 kcal/kg if 70 kg)
15. Feezor Chief Roundtable
December 19, 2005 Amino Acids 70 kg man has 10 kg protein
�Lean body mass�
Turnover is 3% per day in the fed state
Largest component is shed enterocytes (gut)
Protein requirement deceases with age
Protein requirement in adults: 0.8g/kg
60g per day
Maximal protein-sparing achieved when subjects given 1.5 g/kg per day
4 kcal / g
16. Feezor Chief Roundtable
December 19, 2005 Amino Acids Start at 1 g / kg
Increase to 1.5 g / kg on day #2
Check BUN
Avoid if renal dysfunction
17. Feezor Chief Roundtable
December 19, 2005 Electrolytes Another topic. . . .
�Like steroid tapers� � AKL
Largely, trial and error
Use NaCl, K Acetate
Daily BMPs
Adjust
18. Feezor Chief Roundtable
December 19, 2005 Trace elements Thiamine, folate, selenium
Change Zantac to HAL (150 mg/day)
CHANGE BACK when off TPN
Zinc, vitamin C for healing
19. Feezor Chief Roundtable
December 19, 2005
20. Feezor Chief Roundtable
December 19, 2005 Writing TPN A Case Example
21. Feezor Chief Roundtable
December 19, 2005 Writing TPN: what to know What is the patient�s weight? 70kg
How many calories? 30kcal/kg
How much CHO and Fat? 2/3 & 1/3
How much Protein? 1.5 g/kg
Example�
70kg = 2100 kcal
CHO = 1400 kcal
FAT = 700 kcal
22. Feezor Chief Roundtable
December 19, 2005 Writing TPN: Day 1 Volume?
CHO 1400 kcal = 411 g
FAT 700 kcal = 350 mL
Protein 1.5 g/kg = 105 g
23. Feezor Chief Roundtable
December 19, 2005 Writing TPN: Day 2 Volume?
CHO 1400 kcal = 411 g
FAT 700 kcal = 350 mL
Protein 1.5 g/kg = 105 g