Download
1 / 59
830 likes | 1.92k Views
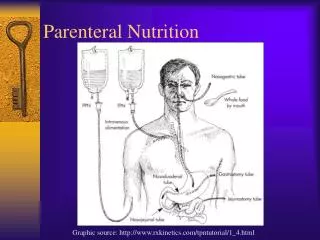
Parenteral Nutrition. PN : a method of feeding patients by infusing a nutritionally balanced & and physico -chemically sterile mixture of all necessary nutrients into the circulatory system, thus bypassing the GIT. Also referred to as: intravenous nutrition,

E N D
PN : a method of feeding patients by infusing a nutritionally balanced & and physico-chemically sterile mixture of all necessary nutrients into the circulatory system, thus bypassing the GIT. Also referred to as: intravenous nutrition, parenteral alimentation, and artificial nutrition.
THE GOLDEN RULE OF NUTRITION The gut should always be the preferred route for nutrient administration. • Enteral nutrition is delivered directly to GIT : • By mouth • By nasogastric tube • By nasoduodenal tube • By nasojejunal tube • By feeding gastrostomy or jejunostomy/ for long feeding only
Therefore, parenteral nutrition is indicated generally when there is severe gastro-intestinal dysfunction(patients who cannot take sufficient food or feeding formulas by the enteral route) .
Categories of PN • If enteral feeding is completely stoppedor ineffective, Total Parenteral Nutritionis used (TPN). • If enteral feeding is just “not enough”, supplementation with Partial Parenteral Nutrition(PPN) is indicated.
In well-nourished adults, 7 - 10 days of starvation with conventional intravenous support (using 5% dextrose solutions) is generally accepted, (PPN). • If the period of starvation is to extendbeyond this time, or the patient is not well-nourished, Total Parenteral Nutrition (TPN)is necessary to prevent the potential complications of malnutrition.
Total Parenteral Nutrition Indications: Short-term use • Bowel injury, surgery, major trauma or burns • Bowel disease (e.g. obstructions, fistulas) • Severe malnutrition • Nutritional preparation prior to surgery. • Malabsorption - bowel cancer • Severe pancreatitis • Malnourished patients who have high risk of aspiration Long-term use (HOME PN) • Prolonged Intestinal Failure • Crohn’s Disease • Bowel resection
Partial Parenteral Nutrition: PPN can be used to supplement ordinary or by tube feeding esp. in malnourished patients. Indications: Short bowel syndrome Malabsorption disorders Critical illness or wasting disorders
Enteral versus parenteral nutrition • As far as gastrointestinal failure is concerned, long term parenteral nutrition is a life-saving procedure. • Enteral nutrition has the advantage over parenteral nutrition of lower % of infectious complications. • Parenteral nutrition has been shown to lead to changes in intestinal morphology and function and an increase in permeability (with higher % of bacterial translocation)
Nutritional Requirements A combination of 6 main groups of nutrient with water: • Energy: Glucose Lipid • Amino acids (Nitrogen) • Water & Electrolytes • Vitamins • Trace elements
Requirements: • Energy • Basal energy requirements are a function of the individual's weight, age, gender, activity level and the disease process. • The estimation of energy requirements for parenteral nutrition relies on predictive equations. • Hospitalized adults require approximately 25-30 kcal/ kg/day. • However, these requirements may be greaterin patients with injury or infection.
Energy Sources: Glucose • The most common source of parenteral energy supply is glucose, being: • Readily metabolized in most patients, • provides the obligatory needs of the substrate , thus reducing gluconeogenesis and sparing endogenous protein. • 1 g of anhydrous glucose gives 4 Kcals. • Most stable patients tolerate infusion rates of 4-5 mg.kg-1.Min-1, but insulin resistance in critically ill patients may lead to hyperglycemia even at these rates, so insulin should be incorporated according to blood sugar levels.
Requirements: • Energy Sources: Glucose Route • Glucose in 5%solution can be safely administered via a peripheral vein, but higher concentrations require a centralvenous line. • 20, 25, or even 50 % solutions are needed to administer meaningful amounts of energy to most patients for proper volume administration.
Requirements: • Energy Sources: Lipid (as fat emulsion) • Fat mobilization is a major response to stress and infection. • Triacylglycerols are an important fuel source in those conditions, even when glucose availability is adequate. • Need to be restricted in patients with hypertriglyceridemia.
Requirements: • Energy Sources: Lipid (as fat emulsion) • Lipids are also a source for the essential fatty acids which are the building blocks for many of the hormones involved in the inflammatory process as well as the hormones regulating other body functions. • Ideally, energy from fat should not exceed 40% of the total (usually 20-30%).
Requirements: • Energy Sources: Lipid (as fat emulsion) • Fat emulsions can be safely administered via peripheral veins, provide essential fatty acids, and are concentratedenergy sources for fluid-restricted patients. • They are available in10, 20 and 30% preparations. • The licensed lipid emulsions types: • Soybean oil • Olive oil / soybean oil combination • Triglyceride (MCT, LCT, & STG)
Dual energy Combination of lipid & glucose; to minimize the risk of given too much lipid or too much glucose, since complications increased if the metabolic capacity of either is exceeded.
Requirements: • Nitrogen • Protein (or amino acids) is the functional and structural component of the body. • 20 types of a.a. are required, 8 are considered essential a.a. • Protein requirements for most healthy individuals are 0.8 g/kg/day • Critically ill patients may need as high as 1.5-2.5 g/kg/day depending on the disease process: (major trauma or burn > infection or after surgery > standard) • Protein required is prescribed in term of nitrogen; 1 g nitrogen equevalent to 6.25 g. protein. • The amount should be reduced in patients with kidney or liver disease.
Requirements: • Nitrogen Daily Protein requirements
Requirements: • Nitrogen • Parenteral amino acid solutions provide all known essential amino acids. • The nitrogen lost in urine derives primarily from amino acids released by protein breakdown in response to catabolic mediators that include stress hormones (corticosteroids, catecholamines) and cytokines. • It is a way to assess the sufficiency of protein intake for the patient.
Requirements: • Nitrogen • Special a.a. solutions are also available containing higher levels of certain a.a.s, most commonly the branched-chain ones (valine, leucine and isoleucine), aimed at the management of liver diseases, sepsis and other stress conditions. • Conversely, solutions containing fewer a.a.s (primarily the essential ones) are available for patients with renal failure.
Requirements: • Nitrogen • Arginine was added to enteral formulae claiming positive effects on immune function and length of hospital stay. • In some clinical trials, glutamine-enriched solutions improved nitrogen balance andgut morphology.
Requirements: • Fluids and electrolytes
Requirements: • Fluids and electrolytes • Normalization of acid-base balance is a priority and constant concern in the management of critically ill patients. • Most electrolytes can be safely added to the parenteral amino acid/dextrose solution. • Sodium bicarbonate in high concentrations will tend to generate carbon dioxide at the acidic pH of the amino acid/glucose mix. • Daily lab tests to monitor electrolyte status
Requirements: • Vitamins • Multivitamin formulations for parenteral use for adult patients usually contain 12 vitamins at levels estimated to provide daily requirements. • Vitamins are either fat soluble (A,D,E,K) or water soluble (B,C). Separate multivitamin commercial preparations are now available for both. • Most adult vitamin formulae do not contain vitamin K, which is added according to the patient’s coagulation status.
Requirements: • Trace elements • Zinc, fluorine, mang., iodine, cobalt, iron, sel., molb., & chromium. • These are essential component of the parenteral nutrition regimen, play a role as co-factor & co-enzyme • A multi-element solution is available commercially, and can be supplemented with individual minerals. • may be toxic at high doses. • Ironis excluded, as it alters stability of other ingredients. So it is given by separate injection (iv or im).
Requirements: • Trace elements • minerals excreted via the liver, such as copper and manganese, should be used with caution in patients with liver disease or impaired biliary function.
Application: • The Solution • Manually mixed in hospital pharmacy or nutrition-mixing service, • premixed solutions, • Separate administration for every element alone in a separate line.
Application: • Venous access • PPN: (<900 m.osmol/L): a peripheral line can be enough. • TPN: Central venous access is fundamental, Ideally, the venous line should he used exclusively for parenteral nutrition. Catheter can be placed via the subclavianvein, the jugularvein (less desirable because of the high rate of associated infection), or a long catheter placed in an arm veinand threaded into the central venous system (a peripherally inserted central catheter line) Once the correct position of the catheter has been established (usually by X ray), the infusion can begin.
Selection of PN line • Peripheral line • short term use • mildly stressed patients • low caloric requirements • needs large amounts of fluid • contraindications to central TPN • Limited to 800 to 900 mOsm/kg (or 1150 mOsm/kg with lipid in the solution) • Dextrose limited to 5-10% final concentration and amino acids 3% final concentration • Limited electrolytes
Type of preparation 2 in One PN 3 in One PN
3 in One (Total Nutrients Admixture) NUTRITION NOTE
3 in One (TNA) • Advantages of TNA • Decreased nursing time • Decreased risk of touch contamination • Decreased pharmacy prep. time • Cost savings • Better fat utilization in slow, continuous infusion of fat • Physiological balance of macronutrients
3 in One (TNA) • Disadvantages of TNA • Diminished stability and compatibility • IVFE (IV fat emulsions) limits the amount of nutrients that can be compounded • Limited visual inspection of TNA; reduced ability to detect precipitates
Application: • Initiation of Therapy TPN infusion is usually initiated at a rate of 25 to 50 mL/h. This rate is then increased by 25 mL/h until the predetermined final rate is achieved. • Administration To ensure that the solution is administered at a continuous rate, an infusion pump is utilized to administer the solution. In hospitalized patients, infusion usually occurs over 22-24 h/day. In ambulatory home patients, administration usually occurs overnight (12-16 h).
Stability • TPN solutions are extremely complex • Components are stable for long time when they are separated, but upon mixing in single container, incompatibilities are present, like: • a.a. are very stable alone or when mixed, but may oxidized when exposed to air & light (glutamine) • Fat emulsions in the mixture are affected by low pH, nature of a.a., electrolyte content, & the total composition of mixture.
Stability • Vit. A & vit. E oxidized by light • Vit. C rapidly oxidized, & may form oxalate stone in the presence of copper ( used with O2 barrier bag) • In general; All TPN solution are stable for 3 months when they are vitamin-free, & should be used within 24 hrs. when mixed with vitamins.
TPN in specific disease state • Hepatic diseases • High rate of infusion of aromatic a.a. increase the risk of cholestasis & encephalopathy (BCAA is preferred) • Reduced clearance of trace element(copper&mang) • Low Na& low volume feeds are indicated in ascites. • Lipid soluble vitamins, zinc & selenium should be considered.
TPN in specific disease state • Renal diseases • Conc. formulation are required; with high energy a.a. & lipid emulsion, high dextrose conc. (Insulin as required), & low electrolyte. • Essential a.a. is reqiured for acute RF but not CRF. • Nitrogen restriction may e necessary for uraemic patients. • Renal clearance of trace elements is reduced (zinc, sel., fluoride & chromium)
TPN in specific disease state • Cardiac diseases • Limited volume of PN, with more conc. Formula is required • Close electrolyte monitoring is required mainly n patient receiving diuretics, ACE-I or digoxin.
TPN in specific disease state • Respiratory dysfunction • Patients with resp. dysfunction or mechanical ventilation, or those can not excert CO2 may have resp. acidosis • Overfeeding may compromise resp. function due to increase CO2 & lipid effects on circulation. • Underfeeding also compromise resp. effort and muscle function • K, Ca, & ph. depletion may worsen resp. & muscle function
TPN in specific disease state • Diabetes mellitus • Insulin is used to manage blood glucose rather than reduce the nutritional provision of the fed. • Insulin should not included within PN formulation due to stability problems & variable absorption rate may required. • Extra K & ph may be required due to the impact of glucose & insulin • Usually; dual energy regimen is indicated
Pharmaceutical Care in TPN • Development nutritional care plan • Care plan includes • Objectives of nutritional support • Method use to provide nutritional support • Indicators of improvement, complications, etc • Educational plan for the patient and caretaker
Monitoring • Policy: to monitor: 1-Effecacy: electrolytes (S. Na, K, Ca, Mg, Cl, Ph), acid-base, Bl. Sugar, body weight, Hb. 2- Complications: ALT, AST, Bil, BUN, total proteins and fractions. 3-General: Input- Output chart. 4- Detection of infection: Clinical (activity, temp, symptoms) WBC count (total & differential) Cultures
Monitoring Monitoring
Pharmaceutical Care in TPN • Monitoring – process of ensuring patient achieves the desired outcome. • Pharmaceuticals related monitoring • Physical appearance of the TPN solution • Color • Gas • Precipitate • Haze / cloudy • Catheter • Precipitate • Leak • Erythema • Rate of infusion • Changes in the rate of infusion should be notified