Download
1 / 45
990 likes | 2.82k Views
Basics of Parenteral Nutrition. Marianne Duda, MS, RD, LD/N, CNSC National Director, Nutrition Program CarePoint Partners, a BIOSCRIP company. History of Parenteral Nutrittion. 1930’s - 1st use of IV glucose 1940’s - 1st use of IV protein hydrolysate 1957 - 1st use of IV lipid

E N D
Basics of Parenteral Nutrition Marianne Duda, MS, RD, LD/N, CNSC National Director, Nutrition Program CarePoint Partners, a BIOSCRIP company
History of Parenteral Nutrittion • 1930’s - 1st use of IV glucose • 1940’s - 1st use of IV protein hydrolysate • 1957 - 1st use of IV lipid • 1969 - 1st human fed with parenteral nutrition • 1979 - 1st home PN patient • 1983 - FDA approved TNA
Indications For PN • Non-functional GI tract • Temporary or permanent failure of enteral feeding • Marginally functional GI tract in the presence of life-threatening malnutrition • Patient refuses enteral feeding
Common PN Diagnoses • Short Bowel Syndrome • Mesenteric Infarct • Bowel Obstruction • Gastric Outlet Obstruction • Fistula • Pancreatitis • Malnutrition • Intractable Vomiting with nausea • Hyperemesis Gravidarum • Radiation Enteritis • Crohn’s Exacerbation • Hypermetabolic state • Malabsorption
Contraindications for PN • Functioning GI tract • digestion • absorption • Aggressive therapy contraindicated • terminal diagnosis (ethics?) • Risks outweigh benefits • Inability to gain venous access
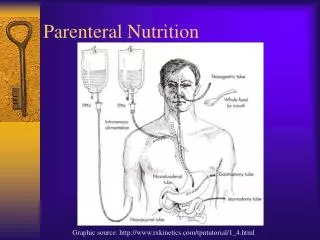
Venous Access • Peripheral • Infused through small veins of the extremities (hands/forearm) • Maximum of 10% dextrose solution • Osmolarity must be < 900 mOsm/L • Short-term therapy only (<2 weeks)
PN Components • Amino Acids • Carbohydrate • Lipids • Electrolytes • Vitamins • Trace Elements • Compatible Drugs • Water
PN Components: AMINO ACIDS • Provided as crystalline amino acids • Provides 4 calories per gram • Function is to maintain nitrogen balance • Requirements vary with clinical condition, usually 1.0-2.0 grams per kg • Available in 3% to 20% concentrations • Disease specific formulations • renal, hepatic, stress
PN Components: CARBOHYDRATE • Commercial carbohydrate • anhydrous dextrose monohydrate in sterile water • Provides 3.4 calories per gram • Maximum oxidation rate • 5mg/kg/min, or 7gms/kg/day • Minimum dose may be 100 -150g/day • Glycerol: dextrose alternative • Provides 4.3 cals/gm
PN Components: LIPIDS • Aqueous emulsions of soybean or safflower oil • Provide essential fatty acids and calories • 10% = 1.1 kcals/ml (250ml = 275 calories) • 20% = 2 kcal/ml (250ml = 500 calories) • 30% = 3 kcal/ml (250ml = 750 calories) • Limit to 1g/kg/day or 25-30% of total Kcal • Give 50-100 grams/week to prevent adult EFAD • Contraindicated with egg allergies • Source of Phosphorus, 7 mM per 500 ml
PN Components: ADDITIVES • Electrolytes • Vitamins • Minerals • Medications • Water
Electrolyte Recommendations Na 1-2 mEq/kg/day K 1-2 mEq/kg/day Ca 10-15 mEq/day (as gluconate) Mg 8-20 mEq/day (as sulfate) Phos 20-40 mmol/day Chloride to maintain acid-base balance Acetate to maintain acid-base balance
PN Electrolytes • Adjusted based on • clinical condition • serum levels and trends • Critical / Acute care • adjust daily • Home care • adjust weekly
Vitamin Recommendations • 6 mg Thiamin* • 3.6 mg Riboflavin • 40 mg Niacin • 600 mcg Folic Acid* • 15 mg Pantothenic Acid • 6 mg Pyridoxine* • 5 mcg Cyanocobalamin • 60 mcg Biotin • 200 mg Vitamin C* • 3300 IU Vitamin A • 200 IU Vitamin D • 10 IU Vitamin E • 150mcg vitamin K* • * FDA recommendations
Trace Element Recommendations • Zinc 2.5 - 4.0 mg/day • Copper 0.5 - 1.5 mg/day • Chromium 10 - 15 mcg/day • Manganese 60 - 100 mcg/day • Selenium 20 - 60 mcg/day • Iodine, Iron, Fluoride and Molybdenum not routinely added
Common Additives • Regular Insulin • H2 Receptor blockers • Cimetidine • Ranitidine • Famotidine • Furosemide • Heparin • Additional vitamins, minerals
Physical Characteristics of PN • Standard Solution • “Two-in-One” • Amino acid and dextrose solution • Uses a 0.22 micron filter • Lipids provided by a separate pump, filter • “Piggy-backed” into the central line
Physical Characteristics of PN • Total Nutrient Admixture (TNA) • “All-in-one” or “three-in-one” • Contains amino acids, dextrose, and lipids • Requires expertise in mixing and storage due to the fragility of the emulsion • Requires larger line filter (1.2 micron) to allow passage of larger lipid molecules
PN Order • Based on established nutritional needs • Determine total calorie, protein, carbohydrate, fat and fluid requirements • Add electrolytes, vitamins, minerals, medications
3:1 Prescription Goal for 67 Kg Adult • 80 GMS AA (800 ml of 10%) • 350 GMS dextrose (500 ml of 70% dex) • 50 GMS lipids (250 ml of 20%) • SWFI QS to 2040ml • Infuse at 85cc/hr • Provides 1690 NPC, 80 gm pro, 2010 Tkcal • 25 npc/kg; 1.2 gm pro/kg; 30tkcal/kg; 30ml/kg • NPC:N ratio = 132:1
3:1 Prescription for 67 Kg Adult • NaCl - 80mEg/day • KAce - 60mEq/day • Kphos - 20 mM/day • CaGlu - 10 mEq/day • Mg So4 - 8 mEq/day • MTE C5 - 1 ml/day • Pepcid - 40 mg/day • Infuvite - 10 ml /Day • Insulin - 35 u/day • 1 unit per 10 grams dextrose • Total compounded volume includes all of above plus overfill, usually about 100ml
Special Considerations • Renal failure • may need to decrease Mg, Phos, K, fluid • Cardiac failure • may need to decrease Na, fluid volume • Short bowel/ileostomy • may need to increase Na, K, Mg, Cl, Zn, fluid • Deficiency states • Refeeding syndrome
Refeeding Syndrome • Over-vigorous feeding of the severely malnourished patient • Dramatic fall in Phos, K and Mg levels • May lead to circulatory collapse and death • Restrict carbohydrate • 2 mg/kg/min or 150-200 gms • Advance carefully over one week • Monitor labs, weight and fluid tolerance • Consider hydration w/lytes before PN initiation
PN Administration Continuous • Used in critical/acute/sub-acute settings • 24 hour infusion • Coexisting diseases, such as diabetes, renal or cardiac diseases, may require continuous infusion
PN Administration Cyclic • typically 10-16 hour infusion mimicking the circadian cycle of eating and fasting • less taxing on the endocrine system, may reduce hepatic complications • may improve quality of life • “the norm” for home care
Cyclical PN • Begin when patient has demonstrated tolerance to final solution and hourly rate • Shorten the infusion period by 4 hour increments, reaching goal in 2-3 days • Decreased time = Increased infusion rate • Taper PN at start and end of infusion, usually over 1-2 hours • Programmable pumps for home care
Monitoring Guidelines Clinical - home environment • Daily nursing visits for the first 4-5 days • assure appropriate support system • teach catheter maintenance, exit site care, infusion techniques and trouble-shooting guidelines; assess patient +/or care partner for compliance • assess catheter site, fluid balance (weight, edema) and vital signs; blood draws prn • Compliance monitoring
Monitoring Guidelines Nutritional - home environment • Nutritional Assessment should be performed within the first week of therapy initiation • Status reviewed weekly by team members • Monthly NST monitoring, then PRN • Team follow-up q six months once stable
Monitoring Guidelines Metabolic • Baseline: CMP, Mg, Phos, (pH) CBC, PT,PTT • Glucose: (FBS <200) • continuous: daily during adjustment phase • cyclic: BS 2 hrs after start and 30 min after end; then prn once stable • Electrolytes / BUN / creat: 2x/week during adjustment phase until stable
Monitoring Guidelines Metabolic (cont.) • CMP/CBC/Mg/P weekly during adjustment phase • Triglycerides: 8-10 hrs after cessation of first lipid dose; then weekly during adjustment phase • LFTS: weekly x one month, then monthly, quarterly • I/O, temperature and weight: daily
Long-term Monitoring Guidelines • Long-term home PN (>90 day duration) • labs: Q 3 month: CMP, Mg, Phos, CBC • Weight • Site care • Micronutrient deficiency • Compliance monitoring • supply usage • solution inventory • Monthly assessment of goals by NST
PN Complications • Nutrient Infusion Complications • Line Complications
Nutrient Infusion Complications • Metabolic • Fluid and Electrolyte Imbalances • Phos, K, Na, Ca, Cl, Mg • Altered Glucose Metabolism • Hyperglycemia: glucose >200mg • Minimize carbohydrate load • add insulin • don’t advance until controlled
Nutrient Infusion Complications • Metabolic • Altered Lipid Metabolism • Hypertriglyceridemia • decrease lipid volume or frequency • increase lipid infusion time • Overfeeding • Hypercapnia • keep calories <40 kcals/kg • reduce carbohydrate load
Nutrient Infusion Complications • Metabolic • EFAD • Provide 10-15% total calories from lipids • Metabolic Bone Disease • Urinary Calcium losses • Aluminum toxicity • Excess vitamin D • Manganese Toxicity • Aluminum Toxicity • Refeeding Syndrome
Nutrient Infusion Complications • Gastrointestinal • Hepatic Dysfunction (Hepatic Congestion, Fatty Liver) • reduce carbohydrate load • cycle PN • avoid overfeeding • L-Carnitine? • Cholestasis • trial of cholecystokinin • trial of glutamine • encourage oral intake • avoid overfeeding
Nutrient Infusion Complications • Gastrointestinal • GI atrophy • transition to oral or enteral feeds as tolerated • Gastric hyperacidity • treat with H2 receptor antagonists
Nutrient Infusion Complications • Particulate contamination • Solid precipitates: Ca and Phos • Phase separation creaming and cracking • Erroneous final concentrations • Microbial contamination of formula
Line Complications • Catheter • Infectious • Culture site and start empirical antibiotics • Sepsis: • Remove catheter and insert new access at another site • Provide antibiotics
Line Complications • Mechanical • Thrombosis: provide warfarin therapy; remove catheter • Infiltration: remove catheter; warm soaks; raise arm • Occlusion:identify and treat causative agent; remove catheter • Pneumothorax: spontaneous or chest tube placement • Pulmonary embolism: prophylactic warfarin therapy; routine EKG and echo
Transitioning off of PN • Improved Gut function • normoactive bowel sounds • passing of flatus, stool • minimal GI drainage or vomiting • Begin enteral/oral feedings • reduce TPN in increments as oral/enteral tolerance improves • D/C when tolerates 65-75% of oral/enteral calories
PN Complications are preventable Ongoing multidisciplinary planning Ongoing interdisciplinary monitoring It Takes a Team
Summary • Ultimate Indication • non-functioning GI tract • documented inability to tolerate enteral feed • Ethics and Economics • IV access • PN formulation, compounding • PN Administration • Monitoring • goals of therapy • complications
Conclusion • PN has been designated a major medical advance of the 20th Century • Provides all known nutrients to those that would otherwise starve • Safe and efficacious in all health settings • Can be customized to meet individual needs • Future includes using nutrients to modulate disease or conditions