Download
1 / 25
250 likes | 259 Views
3 y/o female with bruising. Well child Gum bleeding with brushing past week No meds URI about two weeks ago CBC w/ smear PT/PTT. Diagnosis?. CBC results H/H 12/36 MCV 80 WBC 6.0 65% Neutrophils 35% Lymphs Plts 5,000 Smear. Platelet Disorders.

E N D
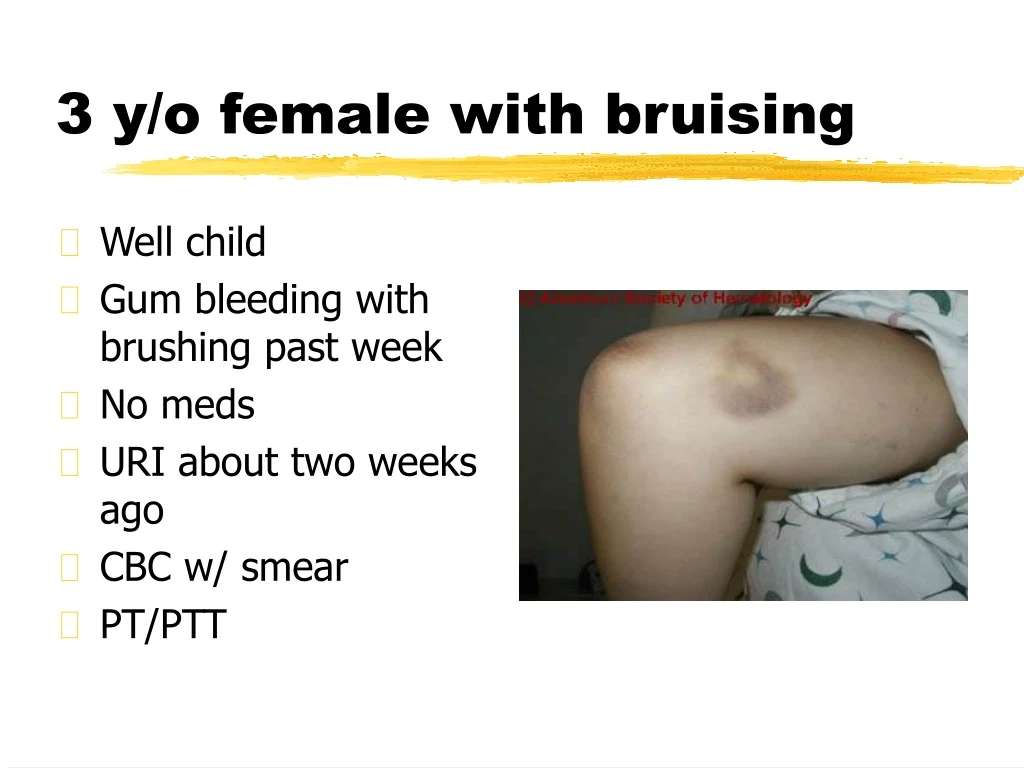
3 y/o female with bruising • Well child • Gum bleeding with brushing past week • No meds • URI about two weeks ago • CBC w/ smear • PT/PTT
Diagnosis? • CBC results • H/H 12/36 • MCV 80 • WBC 6.0 • 65% Neutrophils • 35% Lymphs • Plts 5,000 • Smear
Platelet Disorders Bleeds from skin & mucous membranes (petechiae, purpura, ecchymosis, epistaxis, hematuria, etc.)
Platelet Characteristics • 1-4 microns (young plts are larger) • MPV: 7.1 fl • Number: 150,000-400,000 • Distribution: 1/3 spleen, 2/3 blood stream • Life span: 7-10 days • Lab tests: Plt count, bleeding time (5-12 mins), PFA-100, platelet aggregation studies, plt EM
Classification of Thrombocytopenias • Viral suppression most common • Increased platelet destruction • ITP • Secondary • Infections, drugs, Evans, SLE, etc. • Neonatal ITP
Increased destruction cont’d • Nonimmune thrombocytopenias • Platelet consumption • DIC • HUS • TTP • Kasabach-Merritt syndrome • Cyanotic heart disease • Platelet destruction • Infections, drugs, cardiac
Thrombocytopenia cont’d • Disorders of platelet distribution • Hypersplenism, hypothermia • Decreased production • Hypoplasia • Drugs • Constitutional • TAR; Fanconi’s; Trisomy 13,18 • Marrow infiltrative processes • Storage diseases, leukemias, etc.
Decreased Production • Bernard-Soulier • Autosomal recessive • May Hegglin • Autosomal dominant • Wiskott-Aldrich • X-linked
ITP • Platelet count <100,000 (usually <10,000) • Shortened plt survival (<few minutes) • Antiplatelet antibodies • GP IIb/IIIa, GP Ib/IX, GP V • Not specific for diagnosis • Increased/normal megakaryocytes in bone marrow
ITP • Greatest freq 2-8 y/o • Peak 2-4 y/o • Male = Female • Preceding viral infection within 3 weeks in 50-80% • Life-threatening bleeding uncommon • CNS bleeds in <1%
ITP • Acute • <6 months • Chronic • >6 months • Recurrent
Acute ITP • 50% normal plt count by 2 months • 66% normal plt count by 3 months • 80% normal plt count by 6 months
ITP • Labs • CBC- decreased plts, high MPV • Blood smear- Normal except decreased plts • Consider • Normal PT, PTT • ANA, Complement levels, DAT • Bone marrow aspirate- Not usually needed
ITP Treatment Considerations • Treat or not to treat---?? • Plt counts >35,000 and asymptomatic • No treatment • Avoid contact sports • Wet vs dry purpura
Acute ITP - Treatment • Steroids • 2-4 mg/kg/day for 21 14-21 days with taper • 40-60 mg/day with slow taper • IVIG • 1 g/kg/day for 2 days • WinRho • 50 micrograms/kg x1 • 25 micrograms/kg/day x2
Life-threatening bleed • IVIG 2 gm/kg • Solumedrol 30mg/kg IV (max 1gm) • Platelet transfusion • Factor VIIa • Splenectomy
Chronic ITP • Females > Males (3:1) • Underlying cause often found • Alternate day steroids + IVIG/Winrho • Steroid pulse 4mg/kg/day x4 • Monoclonal anti-CD20 (Rituximab) • Immunosuppressives - VCR, MTX, CTX • Splenectomy • Immunize for pneumococcus, Neisseria, HIB • Pen VK prophylaxis post
Splenectomy for Chronic ITP • Plt count 10-30K and bleeding s/s • Try to wait until 12 months • Continued remissions • Severe lifestyle restrictions • Crippling menorrhagia • Life-threatening hemorrhage • Laproscopic procedure • Accessory spleens






![[PDF] Free Download The Female Brain By Louann Brizendine, M.D.](https://cdn4.slideserve.com/8156681/slide1-dt.jpg)