Download
1 / 1
10 likes | 169 Views
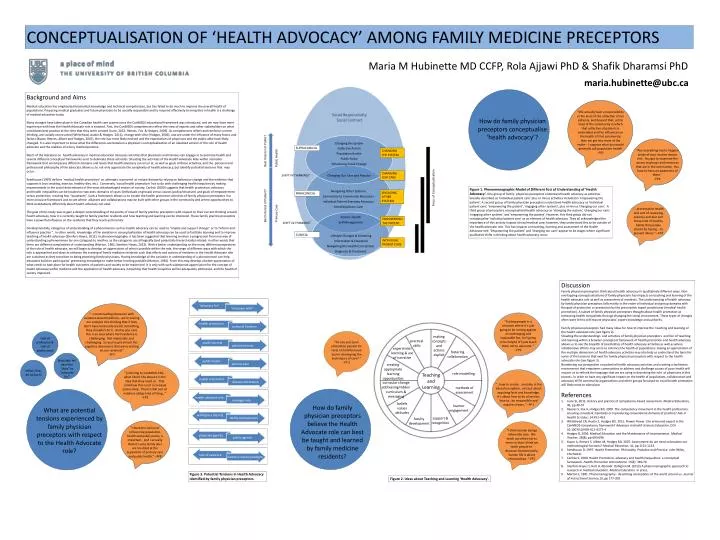
CONCEPTUALISATION OF ‘HEALTH ADVOCACY’ AMONG FAMILY MEDICINE PRECEPTORS. Focus of Conceptualisation. Maria M Hubinette MD CCFP, Rola Ajjawi PhD & Shafik Dharamsi PhD.

E N D
CONCEPTUALISATION OF ‘HEALTH ADVOCACY’ AMONG FAMILY MEDICINE PRECEPTORS Focus of Conceptualisation Maria M Hubinette MD CCFP, RolaAjjawi PhD & Shafik Dharamsi PhD “ [referring to CanMEDS-FM]… what I don’t like about it is the idea that they need us. That somehow this is not a co-equal partnership. There’s that sort of noblesse oblige kind of thing…” –FP2 maria.hubinette@ubc.ca What are potential tensions experienced by family physician preceptors with respect to the Health Advocate role? “advocacy for” “advocacy with” Background and Aims Medical education has emphasised biomedical knowledge and technical competencies, but has failed to do much to improve the overall health of populations. Preparing medical graduates and future physicians to be socially responsible and to respond effectively to inequities in health is a challenge of medical education today. Many changes have taken place in the Canadian health care system since the CanMEDSeducational framework was introduced, and we now have more experience with how the Health Advocate role is enacted. First, the CanMEDS competencies reflect the view of experts and other stakeholders on what constitutes best practice at the time that they were created (Lurie, 2012; Reeves, Fox & Hodges, 2009). As competencies reflect and reinforce current thinking, are socially constructed (Whitehead, Austin & Hodges, 2011), change with time (Hodges, 2006), and are under the influence of many forces and factors (Kuper, Reeves, Albert and Hodges, 2007), the role has most likely evolved and the expectations of physicians and the public alike have likely changed. It is also important to know what the differences are between a physician’s conceptualisation of an idealized version of the role of health advocate and the realities of a busy medical practice. Much of the literature on health advocacy in medical education discusses activities that physicians and trainees can engage in to promote health and several different conceptual frameworks exist to delineate these activities. Situating the activities of the Health Advocate Role within a broader framework that encompasses different domains and levels that health advocacy can occur at, as well as goals of those activities, and the personal and professional philosophy of the advocate allows us to not only appreciate the complexity of health advocacy, but identify potential tensions that may occur. Seedhouse (1997) defines ‘medical health promotion’ as attempts to prevent or reduce disease by relying on behaviour change and the evidence that supports it (not smoking, exercise, healthy diet, etc). Conversely, ‘social health promotion’ has to do with challenging health inequities by making improvements in the social determinants of the most disadvantaged sectors of society. Carlisle (2000) suggests that health promotion, advocacy and health inequalities can be located on two axes: domains of cases (individuals or groups) versus causes (policy/structure) and goals of empowerment versus protection, creating four “quadrants”. Such a framework allows us to situate the health promotion activities of family physician preceptors in a more inclusive framework and to see where alliances and collaborations may be built with other groups in the community and where opportunities to think qualitatively differently about health advocacy can exist. The goal of this study was to gain a deeper understanding of the points of view of family practice preceptors with respect to their current thinking around health advocacy, how it is currently taught to family practice residents and how teaching and learning can be improved. These family practice preceptors have a powerful influence on the residents that they teach and mentor. Developmentally, categories of understanding of a phenomenon such as health advocacy can be used to “enable and support change” or to “inform and influence practice “. In other words, knowledge of the variation in conceptualisation of health advocacy can be used to facilitate learning and to improve teaching of health advocacy (Stenfors-Hayes, 2012). In phenomenography, it has been suggested that learning involves a progression from one way of understanding a phenomenon (or one category) to another, as the categories are all logically (and potentially hierarchically) related; in other words that there are different complexities of understanding (Marton, 1981; Stenfors-Hayes, 2012). With a better understanding on the many different perspectives of the role of health advocate, we will begin to develop an appreciation of what is possible within the role, the range of different ways with which the role is approached and ideas to enhance the training of family medicine residents such that efforts and actions of residents in the Health Advocate role are sustained as they transition to being practicing family physicians. Having knowledge of the variation in understanding of a phenomenon can help educators build on participants’ preexisting knowledge to make better learning possible (Marton, 1981). From this may develop a better appreciation of what needs to take place for health outcomes of patients and society to be maximised. It is only with such widespread appreciation for the concept of health advocacy within medicine and the application of health advocacy in teaching that health inequities will be adequately addressed, and the health of society improved. “We actually have a responsibility at the level of the collective of our patients, and beyond that, at the level of the community in which that collective of patients is embedded and the influences on the health of that community, then we get into more of the realm-- I suppose what you would generally call population health’ -FP2 health promotion How do family physician preceptors conceptualise ‘health advocacy’? personal freedom Social Responsibility Social Contract public interest patient interest Best Interest of Public? public health primary care SUPRACLINICAL CHANGING THE SYSTEM health orientation disease orientation “Not everything has to happen inside of your routine doctor visit. You got to maximize the access to groups and resources that are in the community. You have to have an awareness of them.” -FP4 CHANGING OUR CARE health advocate role SHIFT IN THINKING? manager role Figure 1. Phenomenographic Model of Different Foci of Understanding of ‘Health Advocacy’. One group of family physician preceptors understand health advocacy as activities broadly described as ‘individual patient care’ plus or minus activities included in ‘empowering the patient’. A second group of family physician preceptors understood health advocacy as ‘individual patient care’, ‘empowering the patient’, ‘engaging other systems’, plus or minus ‘changing our care’. A third group of preceptors conceptualised health advocacy as ‘changing the system’, ‘changing our care’, ‘engaging other systems’ and ‘empowering the patient’. However, this third group did not conceptualise ‘individual patient care’ as an element of health advocacy. They all acknowledged the importance of this activity in good clinical medical care; however, they understood this to be outside of the health advocate role. This has impacts on teaching, learning and assessment of the Health Advocate role. ‘Empowering the patient’ and ‘changing our care’ appear to be stages where significant qualitative shifts in thinking about health advocacy occur. Best Interest of Patient? willingness (desire) ENGAGING OTHER SYSTEMS PARACLINICAL ability (competence) “…countervailing obsession with evidence-based medicine…we’re scaring our acolytes into thinking that if they don’t have hard evidence for something, they shouldn’t do it. And as you said, this is an area where hard evidence is challenging. Not impossible, but challenging. So you’ve got almost this cognitive dissonance that we’re visiting on our residents” -FP7 “…preventative health and sort of reviewing exercise and diet and those kind of healthy habits that people should be having …to prevent illness.” –FP3 physician agenda “I think the notion of influencing population health and public policy, is important. And I actually think it’s why family docs are troubled at the separation of primary care and public health.” –FP8 public agenda EMPOWERING THE PATIENT SHIFT IN THINKING? lack of evidence evidence-based paradigm CLINICAL INDIVIDUAL PATIENT CARE Discussion Family physician preceptors think about health advocacy in qualitatively different ways. Non-overlapping conceptualisations of family physicians has impacts on teaching and learning of the health advocate role as well as assessment of residents. The understanding of health advocacy by family physician preceptors falls mainly in the realm of individual and group domains with the goal of protection or prevention by the prescriptive expert practitioner (medical health promotion). A subset of family physician preceptors thought about health promotion as redressing health inequalities through changing the social environment. These types of changes often were felt to still require physicians’ expert knowledge and authority. Family physician preceptors had many ideas for how to improve the teaching and learning of the health advocate role (see figure 2). Situating the understandings and activities of family physician preceptors and foci of teaching and learning within a broader conceptual framework of health promotion and health advocacy allows us to see the breadth of possibilities of health advocacy activities as well as where collaborative efforts may serve to enhance the health of populations. Having an appreciation of the multiple dimensions of health advocacy activities may also help us understand the basis for some of the tensions that exist for family physician preceptors with respect to the health advocate role (see figure 3). Broadening our perspective on potential health advocacy activities and creating a facilitative environment that empowers communities to address and challenge causes of poor health will require us to rethink the language that we are using in describing the role of physicians in this process. In order to have any significant impact on the health of populations, collaboration and advocacy WITH community organizations and other groups focussed on social health promotion will likely need to take place. References Lurie SJ, 2012. History and practice of competency-based assessment. Medical Education, 46, pp49-57 Reeves S, Fox A, Hodges BD, 2009. The competency movement in the health professions: ensuring consistent standards or reproducing conventional domains of practice? Adv in Health SciEduc; 14:451-453 Whitehead CR, Austin Z, Hodges BD, 2011. Flower Power: the armoured expert in the CanMEDS competency framework? Advances in Health Sciences Education, DOI 10.1007/s10459-011-9277-4 Hodges B, 2006. Medical Education and the Maintenance of Incompetence. Medical Teacher, 28(8), pp690-696. KuperA, Reeves S, Albert M, Hodges BD, 2007. Assessment: do we need to broaden our methodological horizons? Medical Education, 41, pp 1121-1123. Seedhouse D, 1997. Health Promotion: Philosophy, Prejudice and Practice. John Wiley, Chichester. Carlisle S, 2000. Health Promotion, advocacy and health inequalities: a conceptual farmework. Health Promotion International. 15(4): 369-76. Stenfors-Hayes T, Hult H, Abrandt Dahlgren M. (2012) A phenomenographic approach to research in medical education. Medical Education. In press. MartonF, 1981. Phenomenography - describing conceptions of the world around us. Journal of Instructional Science,10, pp 177-200. “Putting people in a situation where it’s just going to be ranting against an unchanging and implacable foe, isn’t going to be helpful It’ll just teach them not to advocate. “ –FP2 “Do you put [your articulated passion for care] on hold because you’re developing the techniques of care? “ -FP 2 role of profession & role of professional “I think human beings inherently care. We teach ourselves not to more so than I think we teach people to. Because fundamentally, human life is about relationships. “-FP2 making concepts and actions explicit language: we have the “duty” to “advocate for” practical skills experiential learning & use of narrative fostering collaboration creating appropriate learning opportunities challenges & complexities role modelling Teaching and Learning curricular change addressing hidden curriculum & messaging methods of assessment beliefs values attitudes learner engagement ethics: first, do no harm “…how to create …morality in the education system…not just about acquiring facts and knowledge. It’s about how to be of service, how to…be responsible and acquire virtues ,” –FP1 support & recognition faculty development How do family physician preceptors believe the Health Advocate role can best be taught and learned by family medicine residents? Figure 3. Potential Tensions in Health Advocacy identified by family physician preceptors. Figure 2. Ideas about Teaching and Learning ‘Health Advocacy’.