Download

1 / 18
180 likes | 204 Views
This study examines the impact of caregiver beliefs in medicine on children's adherence to antiretroviral therapy (ART) and viral suppression. Findings suggest that positive beliefs in medicine among caregivers are associated with improved adherence and viral suppression in children.

E N D
Improved adherence to antiretroviral therapyobserved among children whose caregivers had positive beliefs in medicine. G Abongomera1,2, A Cook3, V Musiime4, C Chabala5, M Lamorde6 , J Abach1, M Thomason3, V Mulenga5, A Kekitiinwa7, R Colebunders2, C Kityo4, A S Walker3 and DM Gibb3on behalf of the CHAPAS-3 trial team 1Joint Clinical Research Centre, Gulu, Uganda; 2University of Antwerp, Antwerp, Belgium; 3Medical Research Council Clinical Trials Unit at UCL, London, UK; 4Joint Clinical Research Centre, Kampala, Uganda; 5University Teaching Hospital, Lusaka, Zambia; 6Infectious Diseases Institute, Makerere University, Kampala, Uganda; 7Baylor-Uganda, Kampala, Uganda.
44 Background and Aims • Good adherence to ART is essential for good clinical outcomes • But children rely on caregivers for medication and measuring adherence is difficult • We investigated caregiver views on medicines, their child’s adherence and viral suppression Caregiver views Childs adherence Viral load
44 Background and Aims • Good adherence to ART is essential for good clinical outcomes • But children rely on caregivers for medication and measuring adherence is difficult • We analysed caregiver views on medicines, their child’s adherence and viral suppression Caregiver views Childs adherence Viral load • We investigated whether views on medicine could be used as a proxy for adherence
44 CHAPAS 3 Trial (2010-14) Age 1 month to 13 years 365 Naïve – no previous ART and ready to start 113 Experienced - 2yrs on ART with VL<50 POPULATION RANDOMISED 1:1:1 d4T + 3TC/NNRTI ZDV + 3TC/NNRTI ABC + 3TC/NNRTI minimum 96 weeks follow-up Conducted in three centres in Uganda and one centre in Zambia TRIAL SITES No significant differences in toxicity between NRTIs over 96 weeks; The trial recommended once daily dosing of ABC for African children due to absence of hypersensitivity and superior resistance profile (in agreement with WHO 2013 guidelines) Outcomes and RECOMMENDATION
44 CHAPAS 3 Trial (2010-14) RANDOMISED 1:1:1 d4T + 3TC/NNRTI ZDV + 3TC/NNRTI ABC + 3TC/NNRTI minimum 96 weeks follow-up Conducted in three centres in Uganda and one centre in Zambia TRIAL SITES Outcomes and RECOMMENDATION
44 Methods • Caregiver views on medicines were measured with the Beliefs in Medicine Questionnaire (BMQ) • Adherence was measured using medication event monitoring systems (MEMS) caps • Adherent day defined as 2 openings more than 8 hours apart ( or 1 opening on OD) • HIV-1 viral load assayed with Roche COBAS Ampliprep/Taqman v2.0 • Samples diluted lower limit of detection <100 copies/ml
44 What is BMQ? • An 18-item validated instrument [Horne et al, 1999] • 10 questions measuring beliefs about specific medicine child taking: • 5 measured belief in the necessity of medicine • 5 measured concern about medicine • Each question had five possible answers ranging from strongly disagree to strongly agree (score 1 to 5) • Thus total scores for each of necessity & concern are 5 to 25 • The necessity-concern score is the difference between the two scores (range -20 to +20): • -20 is minimum belief in necessity and max concern • +20 is maximum belief in necessity and minimum concern • 8 questions measured beliefs about medicines in general Reference: Horne R, Weinman J, Hankins M. The Beliefs about Medicines Questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health 1999; 14, 1-24
44 Methods • Two 4-month periods analysed • Period 1 started at randomisation, for ART naïve children this was start of treatment • Period 2 started one year after randomisation BMQ week 0 or 6 BMQ week 48 or 72 MEMS week 0-18 MEMS week 54-72 VL<100c/ml week 48 VL<100c/ml week 96 Period 1 Period 2 NOTE: different children participated in periods 1 and 2
44 BMQ scores, MEMS & VL data * Difference between period 1 and period 2 among children with values in both
44 BMQ scores, MEMS & VL data * Difference between period 1 and period 2
44 BMQ scores, MEMS & VL data * Difference between period 1 and period 2
44 BMQ scores, MEMS & VL data * Difference between period 1 and period 2
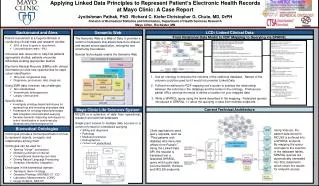
44 Association between BMQ & MEMS β shows effect of 1 unit higher BMQ score on MEMS adherence High necessity score, indicating positive beliefs, associated with better adherence High concern score, indicating negative beliefs, associated with poorer adherence Statistically significant association between Necessity-Concern & Adherence
44 Association between MEMS & VL OR is effect on the odds of viral suppression, with 1% higher MEMS adherence Increase in viral suppression with increased MEMS adherence Statistically significant in period 2, marginally significant in period 1 BMQ MEMS VL<100c/ml
44 Association between BMQ & VL ART naïve at enrolment OR is effect on the odds of viral suppression, with 1 point higher BMQ score OR (95% CI) BMQ scale Period 1 Necessity-Concern 1.02 (0.92, 1.14) Necessity 1.02 (0.81, 1.28) Concern 0.98 (0.86, 1.10) .2 .5 1 2 5 High BMQ score associated with worse VL suppression High BMQ score associated with better VL suppression OR (95% CI) BMQ scale Period 2 .2 .5 1 2 5 Necessity-Concern 1.11 (1.00, 1.24) Evidence of increased VL suppression with higher Necessity, and lower Concern Necessity 1.34 (1.02, 1.77) Concern 0.92 (0.81, 1.06) Statistically significant association between VL and Necessity-Concern in period 2 BMQ VL<100c/ml
44 Conclusions • Caregivers had a strong belief in necessity of ART, outweighing their concerns about treatment. • High levels of adherence to ART were associated with positive overall beliefs towards medicine. • Need of emphasizing necessity of treatment to caregivers, while addressing any concerns they may have about ART • BMQ could be a valuable screening tool used alongside other adherence measures
Acknowledgements Members of the CHAPAS 3 trial team: • University Teaching Hospital, Lusaka, Zambia: Veronica Mulenga, ChifumbeChintu, ChishalaChabala, Desire Kabamba, MusakuMwenechanya, Monica Kapasa, Carol Chijoka, Joyce Lungu, Semy Zulu, Terence Chipoya, Elias Chambela • Joint Clinical research Centre, Kampala, Uganda: Cissy Kityo, Victor Musiime, Grace Mirembe, Elizabeth Kaudha, Amos Drasiku, Bernard Bainomuhwezi, Priscilla Wavamunno, Florence Odongo, Winnie Namala, Daniel Sseremba, Alison Balaba, Alice Kwaga, Joshua Kayiwa, Matthew Odera, Paul Oronon, Edith Bagurukira, Phyllis Mwesigwa, Philip Apugulu • Joint Clinical Research Centre, Gulu, Uganda: George Abongomera, James Abach, Willy Odong, Beatrice Arach • Baylor-Uganda, PIDC, Mulago Hospital, Uganda: AdeodataKekitiinwa, Alice Asiimwe, Vincent Tukei, Violet Korutaro, Justine Komunyena, Carol Nansubuga, MuzamilKisekka, Justine Mpanga • Medical Research Council, Clinical Trials Unit, London, UK: Diana Gibb, Sarah Walker, Margaret Thomason, Adrian Cook, Julia Kenny, Ellen Owen-Powell, Charlotte Male, Adam Glabay • Institute of Child Health, University College London, UK: Nigel Klein, Julia Kenny • Radboud University, Nijmegen, Netherlands: David Burger, QuirineFillekes • University of Cape Town, Republic of South Africa: Helen McIlleron • Trial Steering Committee: Elwyn Chomba, ZainabAkol, Jose Tomas Ramos, Harriet Nakimuli Kyakuha, Cissy Kityo, AdeodataKekitiinwa, Diana Gibb, Veronica Mulenga • Data Monitoring committee: Tim Peto, James Tumwine, Margaret Siwale • Endpoint Review Committee: Hermione Lyall, Diana Gibb, Julia Kenny, Anna Turkova Funder: EDCTP Sponsor: Medical Research Council First-line drugs provided by: Cipla Ltd, India Special thanks to all the children and their families participating in the CHAPAS 3 trial in Zambia and Uganda