Download
1 / 96
1.01k likes | 2.81k Views
Atopic Dermatitis, Eczema, and Noninfectious Immunodeficiency Disorders. Rick Lin, DO MPH July 15, 2003. Atopic Dermatitis. Aka atopic eczema Aka infantile eczema Aka flexural eczema Aka disseminated neurodermatitis Aka prurigo diathsique . Atopic Dermatitis.

E N D
Atopic Dermatitis, Eczema, and Noninfectious Immunodeficiency Disorders Rick Lin, DO MPH July 15, 2003
Atopic Dermatitis • Aka atopic eczema • Aka infantile eczema • Aka flexural eczema • Aka disseminated neurodermatitis • Aka prurigo diathsique
Atopic Dermatitis • High level of IgE antibodies to House dust mites • IgE bound to Langerhans cells in atopic skin • Food exacerbates symptoms in some patients: eggs, peanuts, cow’s milk represent up to 75% of positive test.
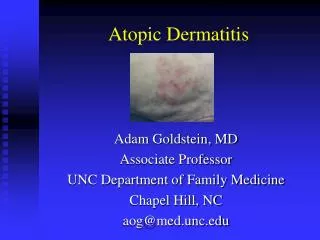
Atopic Dermatitis • Pruritis is the hallmark of AD • Eczematous eruption leads to lichenified dermatitis • Itching precedes the appearance of lesions
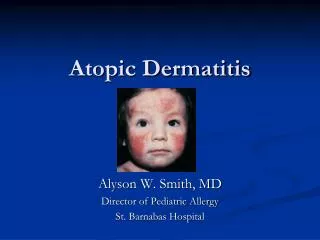
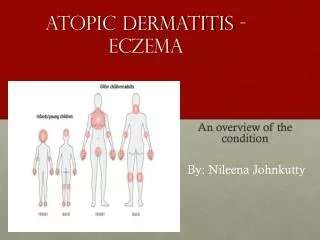
Infantile Atopic Dermatitis • 60% of case AD present in the first year of life, after 2 months of age • Begin as itchy erythema of the cheeks • Distribution include scalp, neck, forehead, wrist, and extensors • May become desquamate leading to erythroderma.
Infantile Atopic Dermatitis • Most cases the symptoms will disappear toward the end of the second year. • The role of food allergy in infantile and childhood atopic dermatitis has been clarified • Egg, peanut, milk, wheat, fish, soy, and chicken may exacerbate infantile AD
Involvement of the cheeks is characteristic of the infantile pattern of AD.
Childhood Atopic Dermatitis • Characterized by less acute lesions • Distribution: antecubital and popliteal fossae, flexor wrist, eyelids, and face. • Severe atopic dermatitis involving more than 50% of body surface area is associated with growth retardation.
Adult Atopic Dermatitis • Distribution: antecubital and popliteal fossae, the front side of the neck, the forehead, and area around the eyes. • Atopic individuals are at greater risk of developing hand dermatitis than are the rest of the population • 70% develop hand dermatitis some times in their lives
Cutaneous stigmata • Dennie-Morgan fold • Pityriasis alba • Keratosis pilaris • Hertoghe’s sign – thinning of the lateral eyebrows • Keratosis punctata palmaris et plantaris
Vascular Stigmata • Headlight sign – perinasal and periorbital pallor • White dermographism – blanching of the skin at the site of stroking with a blunt instrument – cause edema and obscure color of underlying vessels.
Infection • Staph aureus – 90% of chronic lesions • Eczema herpeticum – generalized herpes simplex infection. Young children usually. • Vaccination against smallpox is contraindicated in person with atopic dermatitis. Even when condition is in remission, widespread and even fatal vaccinia can occur.
Immunology • T helper cell type 2 (Th2) dominance • Th2 produces IL-4, 5, and 10 • IL-4 and IL-5 produce elevated IgE and eosinophilia • IL-10 inhibits delayed type hypersensitivity • Th2 maybe sensitive to house mites or grass pollen
Immunology • Monocytes produces elevated amount of prostaglandin E2 (PGE2) • PGE2 reduces gamma-interferon production, but not IL-4 from helper cells thereby enhancing the Th2 dominance • PGE2 also directly enhances IgE production from B cells
Immunology • Langerhans cells of AD patient stimulate helper T cells into Th2 phenotype without the presence of antigen • Langerhans cells have IgE bound to their suface receptors. These IgE are associated with atopic antigens, such as house dust mites
Differential Diagnosis • Seb Derm • Contact dermatitis • Nummular eczema • Scabies • Psoriasis
Histology • Spongiotic dermatitis • Lichen simplex chronicus • Eosinophiles may be seen
Management • Protect from scratching • Adequate cleansing but not over bathing or rubbing • Gentle cleanser • Anti-histamines, especially at night • Bathing protocol • Food allergies concerns and dietary restrictions. • Hydrate skin daily with moisturizers
Management • Topical steroid • Wet compress of Burow’s solution such as Domeboro. • Crude coal tar/liquor corbonis detergens (LCD)
Management • “Topical FK506 (Tacrolimus) is dramatically beneficial in SEVERE atopic dermatitis” • 95% showed good improvement in Alaiti and Rusicka study in JAAD 1998, Archive 1999
Regional Eczema • Ear eczema • Eyelid dermatitis • Nipple eczema • Hand eczema • Diaper dermatitis • Infectious eczematoid dermatitis • Juvenile plantar dermatosis
Ear Eczema • Most frequently caused by seborrheic or atopic dermatitis • Staph, Strep, or Psoeudomonas • Earlobe is pathognomonic of nickel allergy
Eyelid dermatitis • When on one eye only, it is most frequently caused by nail polish • When both eyelids are involved, consider mascara, eye shadow, eyelash cement, eyeline, etc
Nipple eczema • Painful fissuring, seen especially in nursing mothers • Maybe an isolated manifestation of atopic dermatitis • If persist more than 3 month, and/or unilateral, biopsy is mandatory to rule out Paget’s
Hand eczema • Spongiosis histologically • Irritant hand dermatitis- seen in homemakers, nurses. Resulting from excessive exposure to soaps • Pompholyx- tapioca vesicles, on sides of fingers, palms, and soles • Differentials – Bullous Tinea, id, allergic contact dermatitis
Treatment • Barrier • Moisturizer • Systemic Corticosteroids • Phototherapy – UVA, PUVA, Radiotherapy (Grenz Ray)
Diaper dermatitis • Jacquet’s erosive diaper dermatitis • Pseudoverrucous papule and nodules • Graduloma gluteal infantum • Irritation caused by bacteria, change in the environment (wet, lower PH, feces) • Candida albicans are secondary infection.
Infectious eczematoid dermatitis • Vesicular, pustular, or cursted • Ulceration and superficial infection may be present • Treatment involve the removal of irritant and antibiotic treatment.
Juvenile plantar dermatosis • Begins as a patchy symmetrical, smooth, red, glazed macules on the base of the great toes • Affect age 3 to puberty. • Symmetrical lesions on weight bearing area • “toxic sock syndrome” – caused by repeated maceration of the feet by occlusive shoes and nonabsorbent synthetic socks • Virtually always resolve after puberty
Xerotic Eczema • Aka winter itch, nummular eczema, eczema craquele, and asteototic eczema. • Anterior shins, extensor arms, and flank • Elderly person predisposed. • Use of bath oils in bath water is recommended to prevent water loss • Moisturizers – urea or lactic acid.
Nutritional Deficiency Eczema • Localized, thickened pattern with scaling patches. • Exacerbated by nutritional deficiency
Hormone Induced Dermatoses • Autoimmune progesterone dermatitis – urticaria, urticarial paplues, papulovesicular lesion, or eythema multiforme. Appear 5-10 days before menses • Autoimmune estrogen dermatitis – a cyclic skin disorder with variable morphologies. Exacerbate premenstrually or occur only immediately before the menses. Treatment with tamoxifen maybe effective.