Download
1 / 43
430 likes | 573 Views
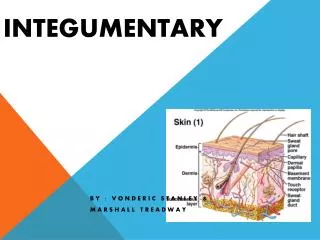
Integumentary Stressors. Increased Risks Caused by Pediatric Differences in the Skin. Skin is thinner, more susceptible to irritants and infection Ratio of skin surface area to body volume is greater, allowing greater absorption More susceptible to bacterial invasion

E N D
Increased Risks Caused by Pediatric Differences in the Skin • Skin is thinner, more susceptible to irritants and infection • Ratio of skin surface area to body volume is greater, allowing greater absorption • More susceptible to bacterial invasion • Less ability to regulate temperature
Common Pediatric Skin Diseases/Disorders • Impetigo • Cellulitis • Candidiasis • Pediculosis • Scabies • Dermatitis • Tinea
Impetigo • Most common bacterial skin infection of childhood • Highly contagious skin infection • Caused by Staph aureus • Incubation 7-10 days • Lesions resolve in 12-14 days with treatment
Clinical Manifestations Lesions appear around mouth and nose Small vesicles initially filled with serous fluid then become pustular Vesicles (bullae) rupture rapidly Honey-colored fluid from lesions becomes crusted mildly pruritic
Nursing Care for a Child with Impetigo • The child can spread impetigo merely by touching another part of the skin after scratching infected areas • Wash the child’s hands frequently with antibacterial soap • Maintain good hand washing • Distract child from touching lesions
Nursing Managementof Lesions • Gently wash lesions 3 times a day with warm, soapy washcloth, crusts carefully removed • Apply topical antibiotic(Bactroban or Bacitracin) • Oral antibiotics effective against staphylococcal and streptococcal organisms • Severe infections treated with IV antibiotics
Parental Education • Good hand washing to prevent spread • Cut child’s nails short, wash hands often with anti-bacterial soap • Do not share towels, utensils with infected child • May return to school or daycare 24 hours after antibiotics started • Finish full course of antibiotics
Candidiasis(thrush) • Superficial fungal infection (Candida albicans) of the oral mucous membranes • May also present in diaper area
Etiology Neonate • can be acquired during delivery if mother has infection Older infant • Immunosupression • during antibiotic therapy, • exposure to mother’s infected breasts • unclean bottles and pacifiers
Oral Thrush White, curd-like plaques on tongue, gums, buccal mucosa (not easily removed)
Diaper Dermatitis Diaper area lesions are bright red Sharp Border Satellite lesions
Management • Nystatin oral suspension applied to mucous membranes • Diaper area treated with topical Nystatin cream
Parental Education • Good hand washing • Thoroughly wash pacifier, bottles • Apply oral Nystatin after feeding to promote increased absorption • Breasts should be treated with Nystatin cream if breast feeding • Watch for spread to GI tract: fever, refusal to eat
Pediculosis CapitisHead lice • Lice can live on a human host for 48 hours • Nits (eggs) capable of hatching for 10 days • Transmitted by direct contact with infected persons or indirect contact with contaminated objects
Clinical Manifestations Nits are visible on hair shafts close to scalp usually behind ears and at nape of neck, difficult to remove Intense pruritis
Management involves three goals • Kill the active lice Kwell, Nix, Rid • Kwell is neurotoxic • Use over the counter pyrethrins (RID) safe and effective • Must treat hair again 1 to 2 weeks after initial treatment • Over the counter pediculicide (NIX) kills head lice and eggs with 1 treatment, has residual activity for 10 days
Management involves three goals • Remove nits • Inspect child’s hair with fine-toothed comb • Comb nits out when hair is wet (apply ½ vinegar ½ water mixture prior to combing) • Prevent spread or recurrence • Treat environmental objects • Examine and treat family members • Vacuum carpets • Check child for reinfestation 7 to 10 days after treatment • Wash all bedding, hats in hot water and high dryer setting • Notify school if reoccurs
Atopic Dermatitis (eczema) • Chronic superficial inflammatory skin disorder • Affects children usually by age 5 yrs • Children usually also have allergies • 75% will develop asthma
Atopic Dermatitis (eczema) Infant: erythematous areas of oozing and crusting on cheeks, forehead, scalp, flexor surfaces of arms and legs Papulovesicular rash and scaly red plaques become excoriated
Atopic Dermatitis (eczema) Childhood: skin appears scaly with dry skin Can be exacerbated by sweating, contact with irritating fabrics, emotional upset
Management • Control pruritis • Bathe with lukewarm water, mild, non-perfumed soap • Applying moisturizer while skin is wet • Anti-inflammatory corticosteroids creams for inflamed areas • Topical immunosuppresants may be used for longer periods of time than topical steroids • Identification and avoidance of allergenic foods
Parental Education • Skin hydration • Support of uncomfortable, irritable child • Mild detergents and soap • Don’t bundle child • Avoid sun exposure • Humidifier during winter months • Avoid drying agents to skin • Fingernails clean and short
Common Types of Tinea Infection • Tinea capitis (scalp) • Tinea cruris (groin, buttocks, and scrotum) • Tinea corporis (trunk, face, extremities) • Tinea pedis (feet)
Tinea Capitis Erythema papular rash of scalp Patches of alopecia Treated with topical and oral antifungals
Tinea Corporis Single circular 1” scaly plaques Erythema to pale pink/white Topical antifungals, continue to treat one week after rash gone
Tinea Cruis Warm moist environment promotes fungal growth Common in adolescent male Topical antifungal Loose clothing
Tinea Pedis Sweaty feet promotes growth Barefoot in common wet areas (pools,lockeroom) Topical antifungal Fresh socks, toss old shoes
Nursing Considerations: All Tinea Infections All members of the family and household pets should be assessed for fungal lesions. Person-to-person transmission is cause Treat all asymptomatic family members for recurrence Good hygiene helps in prevention (don’t share towels, clothing, hats, etc)
Cellulitis Bacterial infection of skin Acute inflammation of dermis and connective tissue Infected area will be edematous, erythematous, very tender, warm-hot May have discharge Enlarged lymph nodes
Treatment Usually associated with elevated WBC Culture will assist in identification of organism Requires aggressive antibiotics May progress into abscess or bacteremia
Nursing Care Warm compresses to the affected area four times daily Elevation of the affected limb if possible Bed rest Administer PO or IV antibiotics Monitor WBC, fever, spread of infection in tissue
Scabies • Mite infection-burrow under skin • Spread by skin to skin contact • Female mite burrows under skin and lays egg • hatch in 3-5 days and cause severe intense itching • Secondary infections (impetigo, cellulitis) common
Clinical Manifestations Intense, severe pruritis esp. at night Papular-vesicluar rash mainly in wrists, fingers, elbows, axilla and groin May see a faint burrow pattern
Management • Elimite- prescription • Application applies neck to toe and must remain on for 8-12 hours • Family members even if asymptomatic and day time contacts should be treated • Wash all bedding, clothing in hot water similar to that for pediculosis
The MD has recommended frequent baths for hydration for a child with eczema. Following each bath, the nurse should: • Apply a light coating of emollient to the child’s skin while still wet • Dry the skin thoroughly and apply baby powder • Dry the skin thoroughly and leave it exposed to air • Apply a dilute solution of 1 part hydrogen peroxide mixed with 9 parts normal saline
Which procedure, performed by parents of an infant with eczema would lead the nurse to realize that additional health teaching is necessary? • Frequent colloid baths • Topical steroid to affected areas • Avoidance of wool clothing • Application of alcohol to crusted area
A preschooler has head lice and must have her head shampooed with a pediculicide that must remain on the scalp and hair for several minutes. How could the nurse best gain this child’s cooperation during the necessary treatment? • Offer the child a reward for good behavior • Inform the child that her parents will be notified if she fails to cooperate • Allow the child to apply the shampoos • Make a game of the treatment “Beauty Parlor”
The nurse is providing home care instructions for a family with a toddler diagnosed with lice, the nurse includes which of the following instructions in the teaching plan? (select all that apply) • Immerse combs and brushes in boiling water for 30-minutes • Vacuum floor and furniture • Have mother use a bright light and magnifying glass to examine the child’s head after lice shampoo • Launder the child’s bedding and clothing in hot water with detergent and dry in a hot dryer for 20 minutes • Shave the child’s head and throw out the hair
Permethrin 5% (Elimite) is prescribed for a 10-year-old child diagnosed with scabies. What instructions should the nurse provide for the mother? • Apply the lotion liberally from neck to toe • Wrap the child in a clean sheet after treatment • Leave the lotion on for 10 minutes then rinse • Apply the lotion only to the child’s scalp
The nurse is caring for a child with cellulitis of the foot. The nurse anticipates the physician ordering: 1. Cold packs BID 2. Application of topical antibiotics 3. WBC and culture of infected site 4. Ace wrap foot and ankle
A adolescent female has been diagnosed with recurrent tineacapitis. The nurse should discuss the impotence of not sharing her friends: 1. Hats 2. Bathing suits 3. Shirts 4. Socks