Download
1 / 44
440 likes | 693 Views
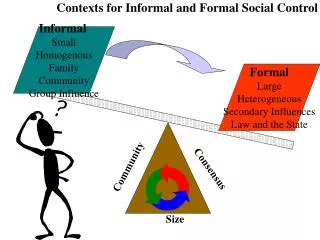
Community Matrons. June 2007. Community matrons: the aim. Improve health outcomes for people with long term conditions Offer a personalised care plan for vulnerable people most at risk Reduce emergency bed days by 5% by 2008 (2003/4 baseline) Improving care in primary and community settings.

E N D
Community Matrons June 2007
Community matrons: the aim • Improve health outcomes for people with long term conditions • Offer a personalised care plan for vulnerable people most at risk • Reduce emergency bed days by 5% by 2008 (2003/4 baseline) • Improving care in primary and community settings
The current situation People with long term conditions: Account for 80% GP consultations 50% of medicines prescribed for people with LTCs are not taken People with LTCs take up 10% of inpatients beds, but account for 55% of in-patient days A high proportion of these VHIUs are not on a DN caseload
Referral Criteria • Three or more active long term conditions • Three or more A&E attendances/ unplanned admissions • Top 3% of GP users • PARR score of >50%
Case Management- what we do planning co-ordinating Supporting people with long term conditions managing reviewing
Benefits of Case Management • Client-centred • Improves clients’ functional abilities • Effective use of resources • Brings together primary and social care • Prevents unnecessary admissions • Reduces length of stay in hospital
The Community Matron’s role • Comprehensive assessment • Innovative case management • Advanced clinical skills and medicine management • Marshalling of resources and co-ordinating primary and social care • Patients empowerment opportunities
Key Challenges • Developing a workforce • Competencies, education and training • Supervision and mentorship • Data and information for case finding and risk management • Systems change and integration with other services
NHS modernisation and the Case Management approach (2) • Intermediate care • Connecting for health • Single Assessment Process • Extended and supplementary prescribing • AHP role development • New pharmacy contract
Community Matrons “Through the unique combination of comprehensive assessment, proactive clinical intervention, marshalling of resources, assessment of the quality of care and co-ordination of acute primary and social care, enable people with multiple conditions, affecting all areas of daily living to remain in control of their own lives” CNO Bulletin, August 2004
PARR: Background • The King’s fund was commissioned to develop a software tool for use by Primary Care Trusts to systematically identify patients who are at high risk in the future of readmission to hospital via emergency admissions. • The PARR case finding algorithm tool became nationally available from September 2005. • The software package was made freely available to NHS organisations on 1st February 2006. The current software package, PARR+ combines PARR 1 and PARR 2
PARR: How does it work? (1) • Clearly a large share of hospital admissions cannot be prevented or avoided. The PARR case finding algorithm does not identify patients randomly. • PARR uses prior hospital discharge data to identify patients at high risk for re-hospitalisation in the 12 months following a “reference” hospitalisation. • PARR aims to identify patients in real time who have a high probability of subsequent emergency admissions while they are hospitalised for certain “reference” conditions for which improved management may reduce the risk of re- hospitalisation.
PARR: How does it work? (2) • PARR focuses on a range of “reference” conditions (including congestive heart failure, COPD, diabetes) where timely and effective case management can help reduce the risks of hospitalisation. • An emergency hospital admission for a “reference” condition is a “triggering” event. This admission creates a “risk score” for the probability of another admission in the next 12 months. • PARR 1 and PARR 2 both use Hospital Episode Statistics (HES) data to produce a ‘risk score’ showing a patients likelihood of admission within the next 12 months. • Risk scores range from 0 – 100, with 100 being the highest risk.
Identifying Patients with PARR • We identify high risk patients, referred to as Very High Intensity Users (VHIU), and offer them care using a case management approach to provide proactive, co-ordinated and joined-up care in community settings. • Evidence shows that intensive, on-going and personalised case management can improve the quality of life and outcomes for these patients, reducing emergency admissions and enabling patients who are admitted to return home more quickly (DOH 2007). • Community matrons must be targeting resources to the VHIU in order to help reach the PSA target of improving care for patients with long term conditions, and reducing the use of emergency bed days by 5% by 2008 (DOH 2007).
HIDAS • Developed web base information system that acts as a reporting tool for the PCT’s data warehouse • Features include: inpatient and outpatient activity, predictive tool, and long term conditions
Outcomes • Being a new service it is important that we monitor our outcomes to demonstrate our success and inform the development of the service • We have carried out a six month audit from 1st October 2006 to 31st March 2007 • The information represents two caseloads with a total of 57 patients
Age and sex of Patients We accept patients aged 18 and over, but the highest number of patients falls between the 75 and 85 age group. There are slightly more female patients, with a ratio of 27 male: 34 female
Source of Referral Most patients are proactively identified by community matrons, with 30% (18) of patients identified using PARR/ Hidas.
Primary Diagnosis at Referral We often manage patients with several co-existing conditions, but referral is usually triggered by a primary diagnosis
Primary Need for Case Management The community matron role can be divided into four key interventions. This graph shows the distribution of our key intervention.
Prevention of Admission • There is currently much debate about how to define or verify a prevention of admission, i.e. how does one prove that something has been prevented? • We have compared admissions and GP usage before and during case management.
Hospital admissions compared • Comparing the figures before and after case management, a significant reduction in admissions can be seen • From the 57 patients, there were 142 admissions recorded in total in the previous 12 months • Since being case managed, patients have had 31 admissions in 6 months • Of those admissions, 28 were seen to be unavoidable or timely and 3 were preventable
Number of Hospital Admissions There is a significant reduction in admissions for patients during case management compared with prior to case management Over 90% of admissions of patients who are being case managed are unavoidable
Reduction in GP home visits Extrapolating figures from the audit to create a full year effect, case management has reduced the number of GP home visits by 162 visits a year
Measuring potential admission avoidance • Whilst we have gone to lengths to compare admissions before and during case management, we are also documenting occasions where we feel that an admission has been prevented • We have divided these into acute episodes and extended episodes of care that potentially lead to admission avoidance
Reduction to Service Usage following Acceptance onto Caseload Community matrons have orchestrated 39 acute episodes where admission to hospital may have been avoided. Extended episodes of care have potentially prevented 76 admissions
The future • Community matrons around the country have sent feedback to the Department of Health asking for help in qualifying a prevention of admission • A preliminary patient and carer satisfaction survey will be sent to all patients on the caseload this summer • A more detailed 12 month audit will be carried out in November which will include cost saving information
Case Study (1): Introduction • 90 year old gentleman • Medical History of COPD, AF, and Hypertension • Discovered via PARR: PARR score of 86% • Command of the English language poor • Extremely hard of hearing • Lives with his wife, his son, daughter-in-law, and their three young children in a three bedroom council house • Daily care worker visit for washing and dressing • Admissions to hospital in the year prior to Case Management: 6 admissions equalling 39 bed days from April 2005 to April 2006
Case Study (1): Assessment Outcome • Poor understanding of and compliance with medication • Inability to use inhalers and nebulisers properly • Lack of follow up after hospital interventions • Urinary incontinence • Frequent exacerbations of COPD followed by hospitalisation
Case Study (1): Intervention • Referral to Audiology • Use of an interpreter for teaching purposes • Medicines management / Change of medication • Education re use of inhalers, using volumatic, and nebulisers • Organising a course of antibiotics and steroids on repeat prescription • Education re signs and symptoms of exacerbation • Family support
Case Study (1): Outcome • No admissions to hospital in the first 9 months of case management • Improved communication • Proper use of medication, inhalers and nebulisers • Supply of pads for urinary incontinence • Patient and family feel supported • 2 hospital admissions and 10 bed days following case management
Case Study (2) : Introduction • 80 year old man, lives alone • Referred by Rapid Assessment Unit • Fulfilled the criteria because • Impairment in instrumental ADL • 3 or more active LTC • Top 3% of GP users • High risk triggers: falls and living alone • COPD, IHD, Renal impairment, Chronic anaemia, Chronic gravitational oedema, L eye blindness, significant speech impairment, faecal incontinence.
Case Study (2): Prior to case management • In previous 12 months had • 1 admisssion • 1 A&E attendance • 2 ICT care episodes • 13 GP home visits • 6 GP surgery attendances • Main focus of case management was improving social situation, care co-ordination, medicine management, monitoring health and acting as the patients advocate.
Case Study (2): Assessment Outcome • The patient was sleeping in a low cane chair and legs were extremely oedematous, affecting mobility, causing falls and skin breakdown • Breathless and fatigued due to anaemia • Faecal incontinence secondary to high faecal impaction • Poor compliance / understanding of medications • Poor social care due to reduced ability to express his needs and substandard carer input • Social isolation.
Case Study (2): Intervention • Obtained new suitable chair from HES • Referred to ICT OT for aids for bed • Referred to DNs for skin care and compression hosiery • Changed diuretics • Requested carers ensure assistance to bed was provided in evenings • Monitoring of Hb and referral back to RAU for blood transfusion • Introduced medication policy for carers to assist with meds and inhalers • Monitoring of bowels and laxative regime • Wheelchair referral • Referral to day centre, befrienders and good neighbours • Ongoing monitoring of health; bloods, BP, Pulse, temp, chest auscultation, weight, leg measurements. • Ongoing social input; order meals for weekends, liaise with good neighbours, feedback to care agency, act as advocate in complaints to care agency, follow up repairs and modifications to council
Case Study (2): Outcomes • No admissions or A&E attendances in 7 months of case management • 3 GP home visits, CM acts as first port of call • Improved mobility, legs less oedematous • Less patient frustration • No further faecal incontinence or constipation • Better compliance with medications • Improving social situation and care input • Example of where case management may have averted a future admission or crisis: development of postural hypotension (increased risk of falls / injury) when dose of thiazide increased, so dose changed.
Case Study (3): Introduction • 72 year old man • Lives with wife, who is main carer • Referred by elderly care consultant • Fulfilled the criteria because: • 3 or more LTC and 3 or more A&E attendances • Impairment in instrumental ADL • High risk triggers include: exacerbation of LTC • PMH: epilepsy, COPD, aortic stenosis, indwelling urethral catheter
Case Study (3): Introduction contd… • 5 admissions • 2 A&E attendances • 5 + GP surgery attendances • Under care of 5 consultants • Presenting problems: • Catheter bypassing • repeated UTIs • bilateral lower leg pain and oedema, • fluid overload • medicine management.
Case Study (3): Assessment Outcome • Patient and carer had poor understanding about his various medical conditions • Community nurses visiting to re-site catheter (approx every 2-3 weeks), and catheter bypassing most of the time • Lower leg pain and oedema, not responding to analgesia • Attending many different OPA
Case Study (3): Intervention • Liaised with urology consultant and requested review of situation and consideration of a supra-pubic catheter. Also requested review of medication • Wrote to consultants explaining rationalising of care and now under the care of Elderly Care Consultant and CM • Medication review • Educated patient and carer about pts medical conditions and put individual care plans in place. Pt weighs himself daily and reports to CM if increase/decrease in weight. Pt and carer will observe urine output and contact CM if infection suspected. Pt reports any signs/symptoms of epilepsy promptly • CM is first point of contact and then will liaise with appropriate member of the MDT. • CM organised a Doppler and prescribed compression hosiery. • CM liaised with elderly care consultant and arranged for the RAU to administer IV diuretic when weight, leg oedema and abdo distension became a problem
Case Study (3): Outcomes • 1 emergency admission (appropriate, but avoidable) • No GP surgery attendances or home visits. • 1 ECP visit (no action taken) • 1 episode with ICT • Experiences nil bypassing with supra-pubic catheter and DN changes every 12 weeks. • Under the care of 3 consultants. • Regular and planned visits by CM to monitor vital signs, monitor weight, measure abdo, assess pain, monitor epilepsy and offer carer support.
Conclusion “The case management approach to LTCs has the potential to have a great impact on the patient experience and the effective and efficient use of resources”