Download
1 / 1
10 likes | 155 Views
Fig. 1. WBRT alone vs. WBRT+SRS. Fig. 2. WBRT alone vs. OP+WBRT. Fig. 3. WBRT+SRS vs. OP+WBRT. (1) Department of Radiation Oncology University Hospital Lubeck, Germany (2) Department of Radiation Oncology, University Medical Center Hamburg-Eppendorf, Germany

E N D
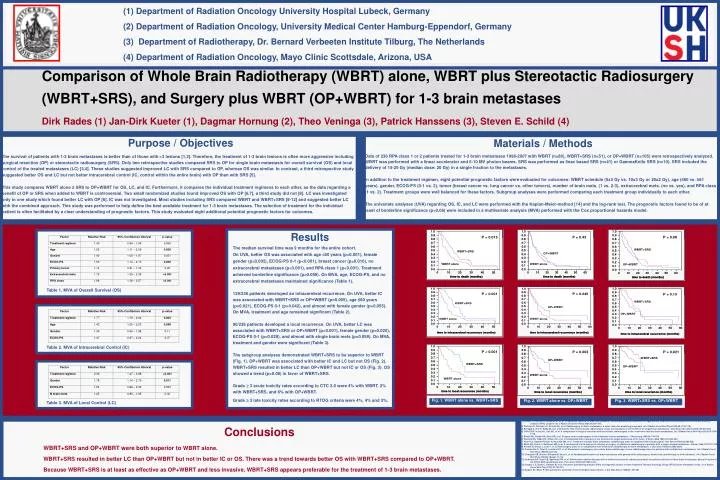
Fig. 1. WBRT alone vs. WBRT+SRS Fig. 2. WBRT alone vs. OP+WBRT Fig. 3. WBRT+SRS vs. OP+WBRT (1) Department of Radiation Oncology University Hospital Lubeck, Germany (2) Department of Radiation Oncology, University Medical Center Hamburg-Eppendorf, Germany (3) Department of Radiotherapy, Dr. Bernard Verbeeten Institute Tilburg, The Netherlands (4) Department of Radiation Oncology, Mayo Clinic Scottsdale, Arizona, USA Comparison of Whole Brain Radiotherapy (WBRT) alone, WBRT plus Stereotactic Radiosurgery (WBRT+SRS), and Surgery plus WBRT (OP+WBRT) for 1-3 brain metastases Dirk Rades (1) Jan-Dirk Kueter (1), Dagmar Hornung (2), Theo Veninga (3), Patrick Hanssens (3), Steven E. Schild (4) Purpose / Objectives The survival of patients with 1-3 brain metastases is better than of those with >3 lesions [1,2]. Therefore, the treatment of 1-3 brain lesions is often more aggressiveincluding surgical resection (OP) or stereotactic radiosurgery (SRS). Only two retrospective studies compared SRS to OP for single brain metastasis for overall survival (OS) and local control of the treated metastases (LC) [3,4]. These studies suggested improved LC with SRS compared to OP, whereas OS was similar. In contrast, a third retrospective study suggested better OS and LC but not better intracerebral control (IC, control within the entire brain) with OP than with SRS [5]. This study compares WBRT alone ± SRS to OP+WBRT for OS, LC, and IC. Furthermore, it compares the individual treatment regimens to each other, as the data regarding a benefit of OP or SRS when added to WBRT is controversial. Two small randomized studies found improved OS with OP [6,7], a third study did not [8]. LC was investigated only in one study which found better LC with OP [6]. IC was not investigated. Most studies including SRS compared WBRT and WBRT+SRS [9-12] and suggested better LC with the combined approach. This study was performed to help define the best available treatment for 1-3 brain metastases. The selection of treatment for the individual patient is often facilitated by a clear understanding of prognostic factors. This study evaluated eight additional potential prognostic factors for outcomes. Materials / Methods Data of 236 RPA class 1 or 2 patients treated for 1-3 brain metastases 1998-2007 with WBRT (n=80), WBRT+SRS (n=51), or OP+WBRT (n=105) were retrospectively analyzed. WBRT was performed with a linear accelerator and 6-10 MV photon beams. SRS was performed as linac based SRS (n=41) or GammaKnife SRS (n=10). SRS included the delivery of 15-25 Gy (median dose: 20 Gy) in a single fraction to the metastases. In addition to the treatment regimen, eight potential prognostic factors were evaluated for outcomes: WBRT schedule (5x4 Gy vs. 10x3 Gy or 20x2 Gy), age (≤60 vs. ≥61 years), gender, ECOG-PS (0-1 vs. 2), tumor (breast cancer vs. lung cancer vs. other tumors), number of brain mets. (1 vs. 2-3), extracerebral mets. (no vs. yes), and RPA class (1 vs. 2). Treatment groups were well balanced for these factors. Subgroup analyses were performed comparing each treatment group individually to each other. The univariate analyses (UVA) regarding OS, IC, and LC were performed with the Kaplan-Meier-method [14] and the log-rank test. The prognostic factors found to be of at least of borderline significance (p<0.06) were included in a multivariate analysis (MVA) performed with the Cox proportional hazards model. • Results • The median survival time was 9 months for the entire cohort. • On UVA, better OS was associated with age 60 years (p<0.001), female gender (p=0.002), ECOG-PS 0-1 (p<0.001), breast cancer (p=0.016), no extracerebral metastases (p<0.001), and RPA class 1 (p<0.001). Treatment achieved borderline significance (p=0.059). On MVA, age, ECOG-PS, and no extracerebral metastases maintained significance (Table 1). • 129/236 patients developed an intracerebral recurrence. On UVA, better IC was associated with WBRT+SRS or OP+WBRT (p=0.005), age ≤60 years (p=0.021), ECOG-PS 0-1 (p=0.042), and almost with female gender (p=0.055). On MVA, treatment and age remained significant (Table 2). • 90/236 patients developed a local recurrence. On UVA, better LC was associated with WBRT+SRS or OP+WBRT (p<0.001), female gender (p=0.020), ECOG-PS 0-1 (p=0.029), and almost with single brain mets (p=0.059). On MVA, treatment and gender were significant (Table 3). • The subgroup analyses demonstrated WBRT+SRS to be superior to WBRT (Fig. 1). OP+WBRT was associated with better IC and LC but not OS (Fig. 2). WBRT+SRS resulted in better LC than OP+WBRT but not IC or OS (Fig. 3). OS showed a trend (p=0.08) in favor of WBRT+SRS. • Grade 3 acute toxicity rates according to CTC 2.0 were 4% with WBRT, 2% with WBRT+SRS, and 6% with OP+WBRT. • Grade 3 late toxicity rates according to RTOG criteria were 4%, 4% and 3%. L Table 1. MVA of Overall Survival (OS) L Table 2. MVA of Intracerebral Control (IC) L Table 3. MVA of Local Control (LC) References [1] Nieder C, Nestle U, Motaref B, et al. Prognostic factors in brain metastases: should patients be selected for aggressive treatment according to recursive partitioning analysis (RPA) classes? Int J Radiat Oncol Biol Phys 2000;46:297-302. [2] Weltman E, Salvajoli JV, Brandt RA, et al. Radiosurgery for brain metastases: a score index for predicting prognosis. Int J Radiat Oncol Biol Phys 2000;46:1155-1161. [3] Schoggl A, Kitz K, Rddy M, et al. Defining the role of stereotactic radiosurgery versus microsurgery in the treatment of single brain metastases. Acta Neurochir (Wien) 2000;142:621-626. [4] O’Neill BP, Iturria NJ, Link MJ, et al. A comparison of surgical resection and stereotactic radiosurgery in the treatment of solitary brain metastases. Int J Radiat Oncol Biol Phys 2003;55:1169-1176. [5] Bindal AK, Bindal RK, Hess KR, et al. Surgery versus radiosurgery in the treatment of brain metastasis. J Neurosurg 1996;84:748-754. [6] Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial of surgery in the treatment of single metastases of the brain. N Engl J Med 1990;322:494-500. [7] Vecht CJ, Haaxma-Reiche H, Noordijk EM, et al. Treatment of single brain metastasis: radiotherapy alone or combined with neurosurgery? Ann Neurol 1993;33:583-590. [8] Mintz AH, Kestle J, Rathbone MP, et al. A randomized trial to assess the efficacy of surgery in addition to radiotherapy in patients with a single cerebral metastasis. Cancer 1996;78:1470-1476. [9] Pirzkall A, Debus J, Lohr F, et al. Radiosurgery alone or in combination with whole-brain radiotherapy for brain metastases. J Clin Oncol 1998;16:3563-3569. [10] Kondziolka D, Patel A, Lunsford LD, et al. Stereotactic radiosurgery plus whole brain radiotherapy versus radiotherapy alone for patients with multiple brain metastases. Int J Radiat Oncol Biol Phys 1999;45:427-434. [11] Chougule PB, Burton-Williams M, Saris S, et al. Randomized treatment of brain metastases with gamma knife radiosurgery, whole brain radiotherapy, or both (abstract). Int J Radiat Oncol Biol Phys 2000;48 (Suppl. 1):114. [12] Andrews DW, Scott CB, Sperduto PW, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. The Lancet 2004;363:1665-1672. [13] Gaspar L E, Scott C, Rotman M, et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys 1997;37:745-751. [14] Kaplan EL, Meier P. Non parametric estimation from incomplete observations. J Am Stat Assoc 1958;53: 457-481. Conclusions WBRT+SRS and OP+WBRT were both superior to WBRT alone. WBRT+SRS resulted in better LC than OP+WBRT but not in better IC or OS. There was a trend towards better OS with WBRT+SRS compared to OP+WBRT. Because WBRT+SRS is at least as effective as OP+WBRT and less invasive, WBRT+SRS appears preferable for the treatment of 1-3 brain metastases.