Download
1 / 51
1.06k likes | 3.08k Views
Dr Ryan Fernandes Asst Professor Department of Surgery. CARCINOMA PANCREAS. INTRODUCTION. Pancreatic cancer is more common in the elderly with most patients being >60 years old. It is more common in African Americans and slightly more common in men than women.

E N D
Dr Ryan Fernandes Asst Professor Department of Surgery CARCINOMA PANCREAS
INTRODUCTION • Pancreatic cancer is more common in the elderly with most patients being >60 years old. • It is more common in African Americans and slightly more common in men than women. • The risk of developing pancreatic cancer is two to three times higher if a parent or sibling had the disease.
Types of Pancreatic Neoplasms • There are three basic types: • Ductaladenocarcinoma >90% of pancreatic cancers with a 4% 5-year survival (worst of any cancer) • Neuroendocrine tumors aka islet-cell tumors, rare • Cystic neoplasms account for <1% of pancreatic cancers
Risk Factors • Established: Smoking, Obesity, and Chronic Pancreatitis. • Possible: DMII, High intake of Fat and/or Meat (particularly smoked or processed meats), physical inactivity
Genetic susceptibility may play a role in 5-10% of cases • Familial history of pancreatic cancer, hereditary cancer syndromes, Peutz-Jeghers Syndromes,BRCA-2 mutations all associated with increased risk of pancreatic cancer
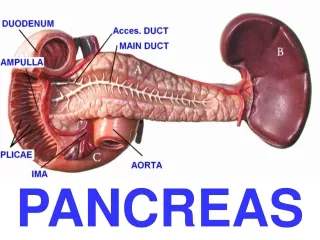
SITES • Head & neck region • Ampullary & periampullary region • Body & tail
Pathology • ≥95% of malignant pancreatic neoplasms arise from exocrine (ductal or acinar) cells • ≈60% arise in head, 15% in body, 5% in tail; in 20% the tumor diffusely involves the entire gland
GROSS APPEARANCE • They appear as hard, irregular, gritty masses that are yellow-gray and are usually poorly demarcated. • They are usually larger than 3 cm in diameter, and both nodal and distant metastases are also frequently present. • Those originating in the body or tail of the pancreas are often larger and more likely to have spread before their presence is known.
MICROSCOPIC APPEARANCE • They are frequently associated with an fibrosis. • Areas of vascular and lymphatic invasion within and around the tumor are commonly seen. • Perineural growth of the tumor is highly characteristic of this cancer and may account for the propensity of pancreatic cancer to extend into neighboring neural plexuses causing both upper abdominal and back pain
SIGNS & SYMPTOMS • Pancreatic cancers are insidious tumors that can be present for long periods and grow extensively before they produce symptoms. • The symptoms, once they develop, are determined by the location of the tumor in the pancreas. • Those in the head or uncinate process of the pancreas make their presence known by causing bile duct, duodenal, or pancreatic duct obstruction.
SIGNS & SYMPTOMS (Contd) Symptoms include – • unexplained episodes of pancreatitis, • painless jaundice, • nausea, • vomiting, • steatorrhea, and • unexplained weight loss • With further spread beyond the pancreas, these patients may note upper abdominal or back pain when peripancreatic nerve plexuses are involved and ascites when peritoneal carcinomatosis or portal vein occlusion develops.
SIGNS & SYMPTOMS (Contd) • Patients with tumors arising in the neck, body, or tail of the pancreas usually do not develop jaundice or gastric outlet obstruction. • Their symptoms may be limited to unexplained weight loss and vague upper abdominal pain until the tumor has grown extensively and spread beyond the pancreas. • New-onset diabetes mellitus is occasionally the first symptom of an otherwise occult pancreatic cancer. • Unexplained migratory thrombophlebitis (Trousseau's syndrome) may be associated with pancreatic and other types of malignancy. • It is a paraneoplastic phenomenon that results from a tumor-induced hypercoagulable state.
Physical Findings • Abdominal Mass or Ascites present in 20% on presentation • Nontender, Palpable Gallbladder (Courvosier’s Sign) may be seen or felt at the right costal margin in those with jaundice • Left SupraclavicularLymphadenopathy (Virchow's node) or a Palpable Rectal Shelf are present in some patients with widespread disease • Hepatomegaly and rarely, Subcutaneous Areas of Nodular Fat Necrosis (Pancreatic Panniculitis) may be evident
Differential Diagnosis • Chronic Pancreatitis/Pseudocyst • Pancreatic Endocrine Tumors • Lymphoma
BLOOD INVESTIGATIONS • Patients with pancreatic head lesions frequently have elevated bilirubin and alkaline phosphatase levels suggestive of obstructive jaundice. • The two most widely used pancreatic cancer serum markers are the CEA and the Lewis blood group carbohydrate antigen CA 19-9. • Both are frequently elevated in patients with advanced disease, but unfortunately, the circulating levels of these tumor markers are often normal in patients with early, potentially curable, tumors.
Investigations • Serology • Radiology • Non invasive:USG,CT,MRI,MRCP • Invasive:Endocopy,EUS,ERCP,FNAC
Imaging Studies • Abdominal US: Dilated bile ducts or the presence of a mass in the head of the pancreas suggest a pancreatic tumor • Helical CT w/o angiography:. Unlike US, can be used for staging • If no mass lesion seen, then ERCP, EUS, or MRI/MRCP may reveal a mass or malignant ductal structures
FNA Biopsy • Preoperative biopsy of a pancreatic mass can be accomplished either percutaneously(US or CT guidance) via EUS or ERCP • Percutaneous: A theoretical concern exists that tumor cells may disseminate intraperitoneally or along the needle path in patients believed to be candidates for potentially curative resection • ERCP: Sensitivity is lower than EUS • EUS: Method of choice, particularly in potential surgical candidates
Need for Pre-op Biopsy • Diagnostic biopsy of a suspected pancreatic malignancy is indicated for treatment planning if there is systemic spread of disease, local evidence of unresectability, or if the patient is unfit for surgery • However, it is controversial whether a pre-op diagnostic biopsy is needed in a fit patient with a potentially resectable pancreatic lesion suspected of malignancy. • While a positive biopsy can confirm the suspected diagnosis, a benign sample does not exclude the presence of malignancy
Adenocarcinoma of the Pancreas: CT scan • What makes a pancreatic mass likely resectable? • No evidence of extrapancreatic disease • Evidence of nonobstructive superior mesenteric-portal vein confluence • No evidence of direct tumor extension to the celiac axis and SMA • EUS, laparoscopy are universally regarded as useful adjuncts to CT, not as essential however
Adenocarcinoma of the Pancreas: CT scan “Borderline” Resectable lesions include: • SMV occlusion of a short segment (open vein proximally and distally) • Body and tail lesions with + celiac, para-aortic nodes in the vicnity • Tumors briefly involving the IVC may be borderline
Pancreatic Cancer Staging • Though TNM staging exists, we can roughly simplify to: • local/resectable, median survival 17 months • locally advanced and unresectable, median survival 8-9 months • metastatic disease, median survival of 4-6 months
Treatment Suspected pancreatic cancer ResectableHelical CT Distant Mets Surgery Locally advanced borderline resectable EUS+FNA ChemoRx EUS+FNA EUS+MRI Palliation ChemoRx Laparoscopy Neoadjuvnt Rx
Treatment • Resectable: surgery +/- adjuvant therapy SURGERY: Pancreaticoduodenectomy (Whipple) Distal pancreatectomy ADJUVANT: chemoradiation(egpost-op 5-FU + gemcitabine)
Locally Advanced: 5-FU chemoradiation • Metastatic: gemcitabine increased survival c/w 5-FU
RESECTION STATUS • R0 – No residual tumor found after resection • R1 – Microscopic residual tumor after resection • R2 – Macroscopic residual tumor after resection
Pre-operative Preparation • Adequate hydration • Glycogen reserve of the liver • Hepatorenal Syndrome – Mannitol • InjVit-K • Antibiotics • ERCP stenting
Criteria for Resection • Tumor size less than 3 cm • Periampullarytumors • Growth not adherent to the portal system
OPERABLE CASES • WHIPPLE’S OPERATION Structures removed – • Tumor • Head & neck of pancreas • C - loop duodenum • Distal stomach • 10 cm proximal jejunum • Lower end of the CBD • Gall Bladder • Lymph nodes
Whipple’s Operation • Choledochojejunostomy • Pancreaticojejunostomy • Gastrojejunostomy
Palliative & Supporting Care: • Endoscopic stenting or surgery bypass for obstruction jaundice or gastric outlet obstruction. • Radiotherapy, opiates and plexus neurolysis for pain.
The Whipple Procedure Pancreaticoduodenectomy - Whipple pancreatic head duodenum gallbladder bile duct +/- gastric antrum
Step 1 - SMV • The inferior border of the pancreas is identified at the level of the proximal body of the gland • The SMV is exposed at the inferior border of the neck of the pancreas, adjacent to the uncinateprocess • The middle colic vein and gastroepiploic vein often arise from a common trunk, which occasionally also involves the right colic vein. • Any or all of these veins may require ligation and division to safely expose the SMV.
Step 2 - Kocherize • A Kocher maneuver can be performed by first identifying the inferior vena cava (IVC) at the level of the proximal portion of the transverse segment of the duodenum (D3) • One can then mobilize the duodenum and pancreatic head off of the IVC in a cephaladdirection.
Step 3 – Porta Hepatis • The common hepatic artery is identified • It is dissected off of the underlying anterior surface of the portal vein • The portal vein is always identified prior to division of the common hepatic duct (CHD)
Step 4 - Antrum • The antrum of the stomach is resected • Jejunum is then transected with a linear gastrointestinal stapler approximately 10 cm distal to the ligament of Treitz
Step 5 - Jejunum • Transection of the jejunum is followed by ligation and division of its mesentery • The loose attachments of the ligament of Treitz are taken down, and the fourth and third portions of the duodenum are mobilized by dividing their short mesenteric vessels
Step 6 - Pancreas • The pancreatic head and uncinate process are separated from the superior mesenteric-portal vein confluence • The pancreas has been transected at the level of the portal vein and the pancreatic head is reflected laterally • allowing identification of small venous tributaries from the portal vein and superior mesenteric vein (SMV) • These tributaries are ligated and divided
…Step 6 • The SMV usually bifurcates into two main branches • one to the ileum • one to the jejunum • Adequate venous return from the small bowel requires that one or the other of these two main SMV tributaries is intact
…Step 6 • Medial retraction of the superior mesenteric-portal vein confluence facilitates dissection of the soft tissues adjacent to the lateral wall of the proximal superior mesenteric artery (SMA) • This site represents the SMA margin • The inferior pancreaticoduodenal artery is identified at its origin from the SMA, ligated, and divided
Step 7 – Pancreaticojejunostomy • The pancreatic remnant is mobilized from the retroperitoneum and splenic vein for a distance of 2 to 3 cm • The transected jejunum is brought up retrocolic through a generous incision in the transverse mesocolon to the left of the middle colic vessels • A two-layer, end-to-side, duct-to-mucosa panceaticojejunostomy is performed over a small Silastic stent
Step 8 - Hepaticojejunostomy • A one-layer, end-to-side hepaticojejunostomy is performed with 4-0 or 5-0 absorbable monofilament sutures distal to the pancreaticojejunostomy • A stent is rarely placed in this anastomosis
Step 9 - Gastrojejunostomy • An antecolic, end-to-side gastrojejunostomy is constructed in two layers • The distance between the biliary and gastric anastomoses should be at least 50 cm • preventing bile reflux cholangitis • prevent possible outlet obstruction caused by the colonic mesentery A No. 10 French feeding jejunostomy tube may be placed distal to the gastrojejunostomy
Step 9- Duodenojejunostomy • Completed reconstruction following pylorus-preserving pancreaticoduodenectomy • The duodenojejunostomy can be placed either retrocolic or antecolic • Prefer an antecolicanastomosis so that there is no potential for obstruction of the jejunum as it exits the transverse mesocolon • Place a jejunostomy tube distal to the duodenojejunostomy because of the concern for poor gastric emptying in the first few weeks following surgery
Conclusion • Poor prognosis • Early diagnosis and treatment