Download
1 / 45
460 likes | 532 Views
Learn about the epidemiology, pathogenesis, pathology, diagnosis, clinical features, and prognosis of carcinoma of the pancreas, the 5th most frequent cause of cancer death. Discover the etiology, morphology, and microscopic features associated with this malignancy.

E N D
CARCINOMA PANCREAS EXOCRINE PANCREASE 5TH MOST FREQUENT CAUSE OF CANCER DEATH PRECEDED BY LUNG,COLON,BREAST PROSTATE CANCER.
CARCINOMA PANCREAS 1.EPIDEMIOLOGY 2. PATHOGENESIS INCLUDING MOLECULAR LEVEL 3.PATHOLOGY GROSS MICROSCOPY 4. DIAGNOSIS 5. CLINICAL FEATURES 6. PROGNOSIS
CARCINOMA PANCREAS EVERY YEAR 28,000 NEW PATIENTS ARE IDENTIFIED. AGE- PEAK INCIDENCEBETWEEN 60 & 80 YEARS
ETIOLOGY OF CARCINOMA PANCREAS 1. HIGHER IN SMOKERS THAN IN NONSMOKERS
ETIOLOGY OF CARCINOMA PANCREAS 2. DIET & OBESITY- HIGH TOTAL CALORIC VALUE,CONSUMPTION OF ANIMAL PROTEINS & FATS. OBESITY IS A RISK FACTOR.
ETIOLOGY OF CARCINOMA PANCREAS 3. CHEMICAL CARCINOGENS-EXPOSURE TO BETA NAPHTHYLAMINE,BENZIDINE, NITROSAMINES
ETIOLOGY OF CARCINOMA PANCREAS 4. DIABETES MELLITUS 5. CHRONIC PANCREATITIS 6. MUTATION IN K-RAS GENE (12p)IS FOUND IN >90% OF CASES. P16 CDKN2A(9p) IN >95% OF CASES P53 (17p) IN 50 – 70 % OF CASES
MORPHOLOGY GROSS- LOCATION – HEAD OF THE PANCREAS 60% OF CASES (20% OF CASES RESECTABLE) FOLLOWED IN DECREASING FREQUENCY BY THE BODY & TAIL 15% IN THE BODY 5% IN THE TAIL 20 % IS DIFFUSE
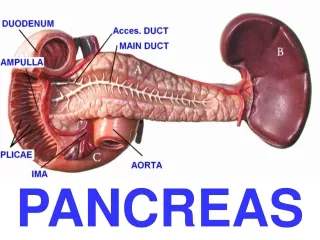
MORPHOLOGY HEAD SMALL HOMOGENOUS POORLY DEFINED GREY WHITE MASS EXTENDING INTO THE AMPULLA OF VATER, COMMON BILE DUCT & DUODENUM- HENCE OBSTRUCT THE COMMON BILE DUCT AS IT COURSES THROUGH THE HEAD OF THE PANCREAS CAUSING MARKED DISTENTION OF THE BILIARY TREE MOST DEVELOP OBSTRUCTIVE JAUNDICE
MORPHOLOGY OBSTRUCTIVE BILIARY SYMPTOMS
MORPHOLOGY CARCINOMA OF BODY & TAIL-LARGE ERREGULAR MASSES ,WIDELY DISSEMINATED BY THE TIME THEY ARE DISCOVERED
MORPHOLOGY CARCINOMA INFILTRATE TRANSVERSE COLON STOMACH, LIVER , SPLEEN , LYMPH NODES (PERIPANCREATIC, GASTRIC,MESENTERIC,OMENTAL AND PORTAHEPATIC ) RETROPERITONEUM ENTRAPPING ADJACENT NERVES ,VERTEBRAL COLUMN.
MICROSCOPY 1.DUCTAL CARCINOMA ADENOCARCINOMA- NO DIFFERENCE BETWEEN CARCINOMA HEAD OF AND BODY AND TAIL OF THE PANCREAS MUCINOUS OR NONMUCINOUS
MICROSCOPY OTHER DUCTAL CARCINOMAS ARE ADENOSQUAMOUS CELL CARCINOMA UNDIFFERENTIATED WITH OSTEOCLAST LIKE GIANT CELL
MICROSCOPY 11. ACINAR CELL CARCINOMA WITH ACINAR CELL DIFFERENTIATION INCLUDING FORMATION OF ZYMOGEN GRANULES AND PRODUCTION OF EXOCRINE ENZYME LIKE TRYPSIN AND LIPASE
MICROSCOPY AND THE PRODUCTION OF EXOCRINE ENZYMES
MICROSCOPY PERINEURAL & INTRANEURAL INVASION
CLINICAL FEATURES OF CARCINOMA PANCREAS DEPEND ON SITE OF ORIGIN OF THE TUMOUR HEAD OF THE PANCREAS- OBSTRUCTIVE JAUNDICE EARLY PRESENTATION
CLINICAL FEATURES OF CARCINOMA PANCREAS DARK URINE,CLAY LIKE STOOLS,PRURITUS,HIGH SERUM ALKALINE PHOSPHATASE.
CLINICAL FEATURES OF CARCINOMA PANCREAS OTHER FEATURES ABDOMINAL PAIN CACHEXIA, ANOREXIA WEIGHT LOSS
CLINICAL FEATURES OF CARCINOMA PANCREAS WEAKNESS,MALAISE, NAUSEA, VOMITING MIGRATORY THROMBOPHLEBITIS ( TROUSSEAU SIGN)
PROGNOSIS DISMAL MEDIAN SURVIVAL IS 6 MONTHS FROM THE TIME OF DIAGNOSIS ONE YEAR SURVIVAL- 10% FIVE YEAR SURVIVAL- 1 – 2 %
INSULINOMA A RARE TUMOUR OF PANCREAS PRODUCE EXCESS INSULIN MORE COMMON IN FEMALES PRODUCE LOW BLOOD SUGAR
INSULINOMA SYMPTOMS OF LOW BLOOD SUGAR ARE TIREDNESS,WEAKNESS,TREMOURS, HUNGER
INSULINOMA PATIENTS HAVE TO EAT FREQUENTLY. SOME PATIENTS DEVELOP PSYCHIATRIC PROBLEMS DUE TO HYPOGLYCEMIA
INSULINOMA USUALLY SMALL LESS THAN 2 Cm 90% ARE BENIGN, ENCAPSULATED RED BROWN MOST ARE SOLITARY
INSULINOMA-MICROSCOPY THE TUMOUR LOOK LIKE GIANT ISLETS WITHOUT MUCH ANAPLASIA IN REGULAR CORD LIKE PATTERN EVEN MALIGNANT TUMOURS ARE DECEPTIVELY ENCAPSULATED
ZOLLINGER-ELLISON SYNDROME(GASTRINOMAS) ZOLLINGER–ELLISON SYNDROME (ZES) IS CAUSED BY A NON–BETA ISLET CELL, GASTRIN-SECRETING TUMOR OF THE PANCREAS THAT STIMULATES THE ACID-SECRETING CELLS OF THE STOMACH TO MAXIMAL ACTIVITY, WITH CONSEQUENT GASTROINTESTINAL MUCOSAL ULCERATION(PEPTIC ULCERS).
ZOLLINGER-ELLISON SYNDROME(GASTRINOMAS) ZES MAY OCCUR SPORADICALLY OR AS PART OF AN AUTOSOMAL DOMINANT FAMILIAL SYNDROME CALLED MULTIPLE ENDOCRINE NEOPLASIA TYPE 1 (MEN 1). THE PRIMARY TUMOR IS USUALLY LOCATED IN THE PANCREAS, DUODENUM .
ZOLLINGER-ELLISON SYNDROME(GASTRINOMAS) HYPERSECRETION OF GASTRIC ACID SEVERE PEPTIC ULCERATION THE RATIO OF DUODENAL TO GASTRIC ULCERATION IS 6:1.
ZOLLINGER ELLISON SYNDROME MICROSCOPIC FEATURES LIKE INSULINOMA –CORDS OF CELLS WITHBLAND FEATURES. RARELY EXHIBIT MARKED ANAPLASIA
ZOLLINGER ELLISON SYNDROME MORE THAN HALF OF GASTRINOMAS ARE LOCALLY INVASSIVE OR ALREADY HAVE METASTASIZED AT THE TIME OF DIAGNOSIS.
ZOLLINGER ELLISON SYNDROME GASTRINOMASMAY BE MULTIPLE WHEN ASSOCIATED WITH MEN SYNDROME1.
MEN SYNDROME MULTIPLE ENDOCRINE NEOPLASIA TYPE 1 (MEN-1 SYNDROME) OR WERMER'S SYNDROME IS PART OF A GROUP OF GENETICALLY INHERITED DISORDERS (HYPERPLASIA,ADENOMAS,CARCINO-MAS)THAT AFFECT THE ENDOCRINE ORGANS KNOWN AS MEN SYNDROME
MULTIPLE ENDOCRINE NEOPLASIA TYPE 1 (MEN-1 SYNDROME) OR WERMER'S SYNDROME COMPONENTS OF THE SYNDROME PITUITARY ADENOMAS, PARATHYROID –HYPERPLASIA+++,ADENOMAS+ PANCREATIC ISLET -HYPERPLASIA++,ADENOMAS++,CARCINOMAS+++) ADRENAL CORTICAL HYPERPLASIA MUTANT GENE LOCUS –MEN1(CHROMOSOME 11q 13)
ZOLLINGER-ELLISON SYNDROME(GASTRINOMAS) 50% OF PATIENTS DEVELOP DIARRHEA. TREATMENT – EXCISION. TUMOURS METASTATIC TO LIVER HAVE SHORTENED LIFE EXPECTANCY