Download
1 / 47
490 likes | 880 Views
Hypersensitivity I & II Ch. 18-19 . March 6th, 2006 Ricky Chang. Objectives. Know the mechanism of Type I hypersensitivity Know the mediators of Type I hypersensitivity Know the diseases associated with Type II hypersensitivity. Hypersensitivity.

E N D
Hypersensitivity I & IICh. 18-19 March 6th, 2006 Ricky Chang
Objectives • Know the mechanism of Type I hypersensitivity • Know the mediators of Type I hypersensitivity • Know the diseases associated with Type II hypersensitivity
Hypersensitivity • Adaptive immunity is important against microbial infections, but it is also capable of causing tissue injury and disease (autoimmune diseases) • Occurs when immune responses are directed against self-ag and also from uncontrolled or excessive responses to against foreign ag, such as microbes and allergens
Hypersensitivity • Common cause is failure of self-tolerance, which ensures that individuals do not respond to their own antigens • Leads to tissue injury that occurs in autoimmune diseases due to the same effector mechanisms used to protect against microbes
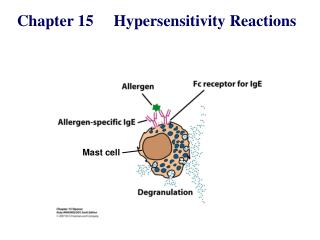
Hypersensitivity • Type I: IgE antibodies bind to Fc receptors on mast cells. IgE induces mast cell degranulation and release inflammatory mediators • Type II: Ab mediated immune response against self antigen or foreign antigen (ie ag on transfused RBC) • Type III: Immune complexes are deposited in tissue • Type IV: T-cell mediated response where Ag sensitized T-cells release lymphokines
Roles of Mast Cells • Part of connective tissue (contains granules of histamine and heparin) • Allergic diseases (asthma,eczema,itch) • Anaphylaxis (systemic shock to allergens such as bee sting,nuts,drugs) • Autoimmune disorders/Acute or chronic inflammation (MS, Rheumatoid arthritis) • Wound healing • Innate response for clearing bacteria and viruses
Mast Cell Basophil
Ag/allergen stimulate CD4+Th2 Th2 releases IL-4, which promote B-cells specific for that Ag to differentiate into IgE producing cells Circulating IgE binds to Fc receptors on mast cells and basophils Elicits a transduction event to release mediators stored in granules (Degranulation) Immediate hypersensitivity response (5-10 minutes) Type I (Immediate)
Type I Mediators and Effects Figure19.3
Type I: Mast Cells • Type I reaction is dependent upon the specific triggering of IgE-sensitizedmast-cells by allergen (Ag) • Ag enter via mucosal surfaces and are taken up by APC • Th2 cells release IL-4 to facilitate the B-cell proliferation and differentiation, producing IgE specific for the allergen • REMEMBER: THIS IS A TH2 RESPONSE!
Activation of Mast Cells • IgE from B-cells binds to FcRI on mast-cells - is the heavy chain responsible for IgE isotype switching • FcRI on mast-cells cross-links with Ag-bounded IgE and induces degranulation of mediators
Cross-linking of FcRI to IgE bounded to Ag Degranulation of Mediators
Activation of Mast-cells Cross-linking
Mast-Cell Mediators • Inflammatory Mediators released -Histamine -Proteases (tryptase or chymase), acid hydrolases -Proteoglycans (heparin, chondroitin sulfate)
Mast Cells: Lipid Mediators • Prostaglandins D2 • Leukotrienes C4, D4, E4 • Platelet-activating factor
Mast-Cells: Cytokines • IL-3: Promote mast cell proliferation • IL-4, IL-5: Promote Th2 differentiation and IgE AB production • TNF-, MIP-1 : Enhance inflammatory reaction
Allergen Induced Hypersensitivity • Allergen: are antigens that induce production of specific IgE AB • Examples: plant pollens, dust, animal hair, animal anti-serum, insect venom, chemicals, and foods • Once the allergen reaches the sensitized mast cells, the allergen crosslinks the surface-bound IgE intracelluar Ca+2 and triggers degranulation of mediators
Atopy • Atopy: Describes individuals that produce IgE AB in response to various environmental Ag and develop immediate hypersensitivity (Type I) responses.(Asthma, eczema, hay fever, and urticaria) • These individuals normally have a strong family history (autosomal transmission of atopy)
Atopy • HLA vs. Allergen Responsiveness -Some allergens response have a relationship to HLA -HLA-DR2 and HLA-A2: high responder to low dos of ragweed -HLA-B8: high responder to ragweed and also associated to other forms of hyperimmunity (autoimmunity)
IgE • IgE blood concentrations are often increased in allergic disease and are grossly elevated in parasitic infections • IL-4: promote B-cells to differentiate into IgE-producing specific cells
Eosinophil • Th2 produce IL-5: Promotes the synthesis and secretion of IgA from B-cells and also important in stimulating eosinophil development and activation • IL-4 and IL-5 production by Th2 cells may account for the eosinophilia seen in type I hypersensitivity and parasitemia
Two Types of Mast Cells • Connective tissue mast cells (CTMCs) • Mucosal mast cells (MMC)
Connective Tissue Mass Cells • CTMCs are found most in blood vessels but vary in size and number of granules at different regions of the body • Diseases such as Crohn’s disease, ulcerative colitis, and RA all present with increase in CTMCs
Types of Fc Receptors for IgE • There are two types of receptors for IgE 1) FcRI (high affinity): Expressed on mast cells and basophils 2) FcRII (low affinity): Expressed by lymphocytes
Mast Cells Activation • Cross-linking can be artificially induced with lectins such as PHA (Polyhydroxyaldehyde) and ConA • These carbohydrates cross-link with IgE and cause degranulation • This explains urticaria in individuals allergic to fruits (ie strawberries-contain large amt of lectin
Degranulation • C’ products of C3a and C5a are very active in degranulating mast cells • Compounds that affect Ca+2 influx into mast cells can induce degranulation • Drugs such as morphine, codeine, synthetic ACTH can create clinical manifestations related to mast cells
Therapy for Allergy 1) Agents that increase intracellular cAMP (-agonist)-inhibits contraction -Theophyllines: Prevents cAMP degradation 2) Blocking mediator release, such as sodium cromolyn: mechanism not clear, but seem to antagonize IgE-induced mediator release.
Therapeutics • Direct Inhibitors -Theophyllines, Xanthines -Sodium cromolyn -Epinephrine -PGE1, PGE2 • Indirect Inhibitor -Glucocorticoids
H1 Bronchial constriction Musous secretion Intestinal smooth muscle contraction Itching and pain at sensory nerve endings H1 and H2 Reduces BP Increase permeability in skin H2 - Gastric secretion in stomach Histamine Receptors
Nausea,vertigo,motion sickness -Cyclizine -Dimenhydrinate -Diphenhydramine (Benadryl, Tylenol PM) -Meclizine H1 Antagonists -Promethazine (Phenergan) -Cetirizine (Zyrtec) -Desloratadine (Clarinex) -Fexofenadine (Allegra) -Loratadine (Claritin) Antihistamines
Type II • Antibodies are directed against ag on particular cells/tissue or extracellular matrix, causing damage (ie RBC transfusion) • These cell- or tissue-specific Ab cause diseases -Myasthenia Gravis: Ab blocks Ach-binding and cause muscle weakness and paralysis -Graves’ Disease: Ab stimulate TSH and casue hyperthyroidism)
Type II • Type II causes disease by 3 mechanism 1) Opsonization and phagocytosis of cells 2) Complement and Fc receptor-mediated inflammation and tissue injury 3) Interference of normal cellular function by binding to important molecules or receptors
Reaction Against RBCs and Platelets • Transfusion Reactions: There are 200 genetic variant of the RBC, but the ABO is the main designation • The Rh system is also important because its cause of hemolytic disease in the newborn
Reaction Against RBCs and Platelets • Hemolytic disease of the newborn (2nd born) -RhoGam: It’s an Anti-Rh+ Antibody given to mother after the first born to prevent future complications in later newborns • Autoimmune Hemolytic Anemia -When provoked by allergic reactions to certain drugs, including Penicillin, quinine, and sulphonamides
Idiopathic Thrombocytpenic Purpura (ITP) • Autoantibody to platelets from the rapid removal of platelets from circulation • Most often develop in women after bacterial or viral infections • Associated with autoimmune disease Systemic Lupus Erythematosus (SLE)
Type II Mediated Autoimmune Diseases • Myasthenia Gravis • Graves’ Disease • Insulin-resistance Diabetes • Hemolytic Anemia • Rheumatoid Arthritis
Advise of the Day TYPE III & Type IV..To Be Continued…