Download
1 / 41
500 likes | 936 Views
IgE Hypersensitivity. Keri Csencsits Smith Department of Pathology and Laboratory Medicine University of Texas Health Science Center at Houston Medical School May 25, 2009 Keri.C.Smith@uth.tmc.edu. Hypersensitivity.

E N D
IgE Hypersensitivity Keri Csencsits Smith Department of Pathology and Laboratory Medicine University of Texas Health Science Center at Houston Medical School May 25, 2009 Keri.C.Smith@uth.tmc.edu
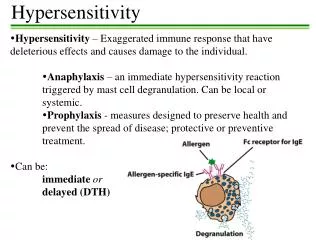
Hypersensitivity • Broad-spectrum inflammatory response that results in significant tissue injury, serious disease, or death • Not necessarily an increased response, rather, an inappropriate response to an antigen. • Hypersensitivity reactions are divided into 4 types
1913 Nobel Prize • Portier and Richet • Coined the term “anaphylaxis” Portuguese Man O’War Booster shot X
Type 1 response (the beginning) • Induced by Allergens • (nonparasitic antigens antigens capable of stimulating type I hypersensitivity reactions) • Distinguished by the secretion of IgE
What leads to IgE response? • Inhaled small protein allergens • Low-dose • Mucosal route of entry
Some enzymes are triggers of allergy Dust mite cysteine protease Der p 1
Class switching to IgE • Remember, this is Th2 mediated • IL-4 is the hallmark Th2 cytokine • IL-13 associated with allergic response
Signaling through the FceR1 Gilfillan et al.Nature Reviews Immunology 6, 218-230 (March 2006) | doi:10.1038/nri1782
9, 9-13(January 2009) | doi:10.1038/nri2458 Don’t forget about basophils! Karasuyama, et al 9, 9-13 (January 2009) | doi:10.1038/nri2458
The usual sequence of events in an allergic reaction is as follows: The allergen combines with circulating IgE, then IgE allergen complex binds to mast cells The allergen binds to IgE fixed to mast cells The allergen is processed by APCs and then binds to histamine receptors The allergen is processed by APCs and then binds to mast cells The allergen combines with IgG B: IgE binds passively to cells expressing high affinity Fc receptors for IgE, then interacts with the allergen when present. The result is mast cell degranulation.
A human volunteer agrees to be passively sensitized for IgE specific for a ragweed antigen. When challenged with the allergen intradermally, he displayed a typical skin reaction due to an immediate hypersensitivity reaction. If the injection with sensitizing IgE was preceded by an injection (at the same site) of Fc fragments of human IgE, followed by intradermal injection with allergen, which of the following outcomes would you predict? No reaction would occur because the Fc fragments would interact with the allergen and prevent it from gaining access to the sensitized mast cells. No reaction would occur because the Fc fragments would interact with the IgE antibodies, making their ag-binding sites unavailable. No reaction would occur because the Fc fragments would interact with the FceR receptors on mast cells The reaction would be exacerbated due to increased local concentration of IgE Fc fragments The reaction would be exacerbated due to the activation of complement C: The soluble Fc fragments would saturate the FceRs, and the allergen specific IgE could not bind to the mast cells.
Phases of the allergic reaction • Immediate • Within seconds • Due to activity of histamines, prostaglandins and the resulting rapid increase in vascular permeability and contraction of smooth muscle • Late-phase • 8-12 hours later • Caused by induced synthesis and release of leukotrienes, chemokines, cytokines from activated mast cells • Induces mucosal edema, mucus secretion, leukocyte infiltration, epithelial damage, bronchospasm • Responsible for the most serious long -term illness
Immediate and late-phase allergic reactions Asthma Wheal-and-flare
Response depends on route of entry and location of mast cells
Chronic inflammation • IL-5 increases production of eosinophils, eotaxin causes them to migrate • Characterized by influx of eosinophils and effector T cells (usually Th2 cytokine secreting) • Persistence of antigen drives further IgE secretion and eosinophilia Eosinophil biology section - NIAID
Consequences of IgE Hypersensitivity • Hay fever • (Allergic rhinitis) • Increase in capillary permeability and localized vasodilation • Food allergies • Smooth muscle contraction and vasodilation leads to diarrhea and vomiting • Wheal and flare (hives) in skin • Allergic dematitis • Inflammatory cytokines cause influx of cells and development of skin lesions • Atopic children often develop prolonged inflammatory response and a persistent skin rash (eczema)
More Consequences of IgE Hypersensitivity • Asthma • Events are: • Reversible airway obstruction • Augmented bronchial responsiveness • Inflammation • Cytokine induced recruitment of inflammatory cells, particularly eosinophils • Cells release oxygen radicals, nitric oxide, cytokines • Leads to development of mucus, edema, sloughing of epithelium
Pathology of allergic asthma Occlusion of airway by mucus plug Inflammatory infiltrate of epithelium
Really bad consequences of IgE hypersensitivity • Systemic anaphylaxis • Can lead to anaphylactic shock • Widespread increase in vascular permeability leads to catastrophic loss of blood pressure • Airways constrict • Epiglottis swells • Usually in response to quick absorption of allergen from the gut (peanuts, brazil nuts), or direct introduction into bloodstream (i.v. drug administration, insect bite)
Factors that contribute to IgE mediated allergy • Genetic • Atopy: the tendency to mount IgE responses to a wide variety of common environmental allergens • As many as 40% in Western populations • Environmental • Exposure to infectious disease in early childhood • Exposure to bacteria in early childhood • Pollution • Allergen levels • Diet
“The Hygeine Hypothesis” • “Dirty” kids have fewer allergies • Growing up on a farm (1999, 2000) • Attended day care (2003) • Pet ownership (1999) • Lower standard of living (East vs. West Germans, 2002)* • Role of bacterial products • Exposure to tuberculosis • Endotoxin exposure • Role of the innate immune system? • PAMPS bind PRR on APC
Toll-like receptors Signaling through TLR expressed dendritic cells up-regulates Th1 cytokines and responses
So why do we have IgE responses? Killing of parasitic worms
Treatment of IgE Hypersensitivity • In use: • Desensitization – increasing doses of antigen drive Th1 response • Antihistamines – block histamine H1 receptor (on blood vessels and on unmyelinated nerve fibers) • Bronchodilators – act on b-adrenergic receptors, relax constricted muscles • Topical or systemic corticosteroids - reduce inflammation • Epinephrine – stimulates reformation of endothelial tight junctions, promotes, muscle relaxation, stimulates heart • Omalizimab (anti-IgE monoclonal antibody)
Treatment of IgE hypersensitivity • Experimental • Vaccination – use peptides derived from common allergens, may induce T cell anergy • CpG adjuvants – promote Th1 responses • Inhibit IL-4, IL-5, IL-13 • Give IFNg or IFNa • Block IgeR1 binding – IgE Fc construct • Block recruitment of eosinophils (anti CCR3)