Download
1 / 20
200 likes | 392 Views
Immersive Virtual Reality as a Rehabilitative Technology for Phantom Limb Experience. Craig D. Murray*†, Stephen Pettifer**, Fabrice Caillette**, Emma Patchick* and Toby Howard** *School of Psychological Sciences, University of Manchester, UK

E N D
Immersive Virtual Reality as a Rehabilitative Technology for Phantom Limb Experience Craig D. Murray*†, Stephen Pettifer**, Fabrice Caillette**, Emma Patchick* and Toby Howard** *School of Psychological Sciences, University of Manchester, UK **School of Computer Science, University of Manchester, UK
Acknowledgement The research reported here is supported by a grant from
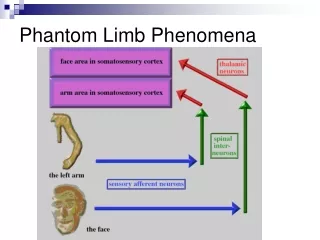
Affects of Phantom Limb Pain (PLP) • Overall adjustment to amputation is impaired as levels of pain increase • Less likely to use a prosthetic limb as levels of pain increase: • Restriction of normal activities • Increased body image dissatisfaction • Higher levels of depression What is Phantom Limb Experience? Phantom sensation: widely accepted as a natural consequence of amputation The experience of the amputated limb as still intact • Phantom Limb Pain (PLP): painful sensations in the phantom limb • Frequency of PLP as high as 85% post-amputation • As many as 70% of phantoms remaining painful up to 25 years after the loss of a limb
? Treating Phantom Limb Pain Pharmaceutical, surgical and psychological interventions have proved to have limited success and longevity in treating PLP • Ramachandran and Rogers Ramachandran (1996) • Mirror placed vertically inside a box with the top removed • Reflection of their remaining anatomical limb in the phenomenal space of their phantom limb • Induced vivid sensations of movement originating in the muscles and joints of their phantom limb • RESULT? Relief from PLP • Control gained over paralysed phantoms
Limitations of the Mirror Box • User must remain oriented towards the mirror: • Few degrees of freedom with movement of their head – need to focus on reflection no matter how large the mirror box is made Illusion is easily shattered by focusing on the intact arm providing the reflection
Virtual Reality! A contemporary, innovative technology that has already been exploited with some success in the amputee population Developing the Mirror Box The mirror box contributes to a converging line of evidence that when feedback of limb movement is manipulated appropriately, it can evoke kinesthetic sensations in that limb More robust visual therapy could potentially prove to provide greater therapeutic benefits than the mirror box:
Immersive Virtual Reality (IVR) Objectives Create a new visual therapy for the treatment of phantom limb pain Aims and Purpose • Produce virtual facsimilies of amputees’ phantom limb which can be controlled by movements of the opposite anatomical limb • Implement appropriate measures to objectively assess the efficacy of using IVR in this way to treat PLP • SECONDARY AIMS: • Implement measures to assess the efficacy of using IVR in this way to: • 1. Decrease body image dissatisfaction • 2. Enable successful prosthesis use
Upper Limb Lower Limb Sensor -Wrist Sensor - Knee Data glove Sensor - Foot Sensor - Elbow For both, Polhemus Fastrak – emits magnetic field to monitor sensors For both, HMD tracks head position and orientation and to present the virtual environment to the eyes and facilitate immersion How Does it Work? In order to transpose movements, we must first be able to track movements:
How Does it Work? Limb Position - Placing constraints on joint angles: • Impossible positions are avoided • Allows minimal sensors to fully ascertain limb position Limb Movement - Joint angles parametisation = ability to transfer from one limb to the other: • Joint angles recovered from active limb • Inverse kinematics applied and transferred to opposite virtual limb • RESULT? Opposite virtual limb ONLY moves but in mirror image motion Real-time transferral of joint angles =responsive fluent motion of virtual limbs Real world points mapped onto virtual world points Calibration - i.e. Area of dance mat calibrated so no mismatch Deformable polygonal mesh attached to the underlying kinematic model for realistic results at a gross level. Detail sacrificed for responsive virtual limbs Body Appearance - Shadows - “Shadow-Map” facility allows shadows to be cast – important for reaslism, sense of immersion and DEPTH PERCEPTION
How Does it Work? Interface on start up allows variations to be achieved at the click of a button :
Potential for Further Development – Benefits of IVR System • Transposition of movement can be more flexible – not just mirror movement • Can implement accurate, objective measures to assess task performance • Representation of the body can be altered to investigate aspects of body image Advantages of the System • Can orient anywhere in the virtual environment – more degrees of freedom of movement in the head • Only target limb (Phantom limb) is seen to move in virtual environment – illusion is more robust • Can engage in one-handed tasks – attention is focused more heavily on target limb
Study Design and Procedure Longitudinal study to assess any change in levels of PLP over time: - Participants attend testing sessions at least once every 2 weeks for a period of 20 weeks (case study interventions also proposed) - Tasks completed in repetitions for 30 minute sessions at a time Between-subjects design Due to the nascent approach of using IVR to treat PLP, a control group is necessary to assess the outcome of treatment over and above any placebo affects: - Experimental Group – visual representation of virtual phantom limb controlled by movements of the opposite anatomical limb - Control Group – visual representation of virtual limb controlled by movements of the corresponding anatomical limb i.e. No transposition of movement carried out Hypothesis –Experimental Group will experience significant short- and long- term reductions in the frequency and severity of PLP whilst Control Group will not. AND Experimental Group will experience significant positive changes in psychosocial issues, activity restriction and satisfaction with a prosthesis, whilst Control Group will not
Participants and Experimental Measures • Participants • Currently being recruited via sub-regional Disablement Services Centre. • 32 amputees = target sample (16 experimental, 16 control) • INCLUSION CRITERIA: • Minimum 12 months post amputation with phantom limb pain • Unilateral, adult amputees • Suitable for being provided with a prosthetic limb • Experimental Measures • The following are completed once, one week prior to using IVR system and again on completion of involvement with study: • The McGill Pain Questionnaire – indicates subjective global PLP experience • The Amputee Body Image Scale –assesses how an amputee perceives and feels about his or her body experience • The Trinity Amputation and Prosthetic Experience Scales – multidimensional self-report instrument to help understand adjustment to an artificial limb
Experimental Measures cont. • Since investigating the change in PLP over time is the primary goal of the research, we also want a continuous assessment of levels of PLP over time: • Short Form MPQ – administered at end of each IVR session • Pain Diaries – brief predominantly numerical diaries completed through course of involvement with study • Due to the highly subjective nature of phantom limb experience, brief semi-structured interviews with individual participants are carried out throughout the testing period to establish the phenomenology of their phantom limb • Covariate, Exploratory Measures for analysis: • Mood Questionnaire – due to the nature of pain in general and it’s variability with emotional disposition, a brief questionnaire to establish mood is carried out prior to each testing session • Vividness of Imagery - measure of participant’s ability to visualise movement in their phantom limb during IVR sessions
Phantom Pain Relief Body Image Disturbance AND Prosthesis Satisfaction Over and above any placebo affects Data Analysis and Future Testing Participants’ scores on the: MPQ,short form MPQ, Pain Diaries ABIS and TAPES Compared over the study period AND between the two VR conditions. This allows assessment of the short- and long- term therapeutic benefits of IVR for… • Transcribed interviews = exploratory qualitative analysis to contextualise the more quantitative findings • Vividness of Imagery Questionnaire and Mood Questionnaire – exploratory covariates in analysis Testing will begin shortly and updates on progress will be posted at: http://aig.cs.man.ac.uk/research/phantomlimb/phantomlimb.php