Download
1 / 32
391 likes | 1.2k Views
Lachrymal system. Prof Dr Rengin YILDIRIM. Lacrimal drainage system. . Tear Production and Drainage. The majority of tears are produced by accessory tear glands located within the eyelid and conjunctiva. The lacrimal gland itself is really only responsible for

E N D
Lachrymal system Prof Dr Rengin YILDIRIM
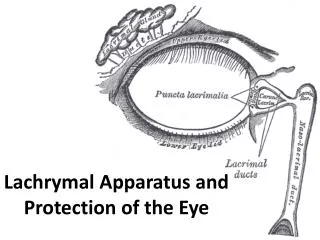
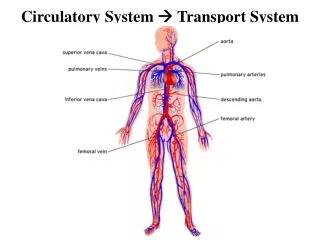
Tear Production and Drainage The majority of tears are produced by accessory tear glands located within the eyelid and conjunctiva. The lacrimal gland itself is really only responsible for reflexive tearing. Tears flow down the front of the eye and drain out small pores, called lacrimalpunctum
Puncta • Each punctum is present at the medial end of both the superior and inferior lid. • They are situated on slight elevations called the lacrimal papillae and face posteriorly so it is necessary to evert the medial lids to inspect them. • Malposition or stenosis (narrowing) of the puncta may cause epiphora.
Vertical canaliculus This is about 2mm long and joins the horizontal canaliculus at a right angle called the ampulla.
Horizontal canaliculus • This is about 8mm long and usually joins its fellow to form the common canaliculus which immediately enters the (naso)lacrimal sac through the Valve of Rosenmuller (flap of mucosa to prevent reflux).
Nasolacrimal sac • This is about lOmm long and funnels into the nasolacrimal duct.
Nasolacrimal duct This is about l2mm long and opens into the inferior nasal meatus, lateral to the inferior turbinate (concha). The Valve of Hasner closes the opening.
Valves • About seven other valves have been described within the nasolacrimal duct besides those of Rosenmuller and Horner (see Last) but they have no valvular function and are usually ignored
PHYSIOLOGY OF THE LACRIMAL DRAINAGE SYSTEM Capillarity ensures that 70% of the tears enter the inferior canaliculus and 30% through the superior . On blinking, the attachment of the preseptalorbicularis muscle helps create positive and negative pressure in the lacrimal sac which sucks the tears into it . This is called the tear pump. Gravity then helps keep the sac empty.
ETIOLOGY OF EPIPHORA • hypersecretion occurs when a foreign body irritates the cornea. • Paradoxically, it may also be due to an underlying dry eye problem which, in turn, causes a foreign body reaction and tearing. • Likewise, it may be due to a lacrimal pump failure as in ectropion when tears are no longer able to enter the punctum. It may also be caused by punctum plugs or punctumcauterisation for the treatment of dry eye.
EVALUATION OF EPIPHORA General inspection Inspect the lids to see if they and/or the puncta are poorly positioned. Palpate the lacrimal sac to determine if it is enlarged due to dacryocystitis or a mucocele. Compression may cause a reflux of mucopurulentmatter. Pain suggests dacryocystitis.
Slit lamp examination • Inspect the puncta for poor position, narrowing or blockage - pouting suggests canaliculitis. • A high marginal tear strip may indicate epiphora. If fluorescein is instilled in the conjunctival sac, it should disappear within two minutes - retention suggests there is a problem with lacrimal drainage.
Hard stop If the cannula touches the medial wall of the lacrimal sac and lacrimal bone, a definite end point is reached. This is a 'hard stop‘ and indicates that there is no complete obstruction in the canalicular system
Soft stop • If a spongy end point is felt, this is termed a 'soft stop’ and indicates that the cannula has been prevented from entering the lacrimal sac. Therefore, there is a blockage in the canalicular system and there will be no distension of the lacrimal sac when the plunger is pressed
Detailed diagnosis from lacrimal syringing • If saline refluxes from the inferior canaliculus, the blockage is there. • If saline refluxes from the superior canaliculus, the blockage is in the common canaliculus. • If saline passes into the nose, the problem is hypersecretion of tears or failure of the lacrimal pump or partial obstruction of the nasolacrimal system. • If saline does not reach the nose, there is a total obstruction of the nasolacrimal duct and saline may appear from the superior punctum - the saline may be purulent if infection is present - and the lacrimal sac may be distended
Functional obstruction • Sometimes, the lacrimal drainage system may appear patent when syringing proceeds uneventfully. • However, there may be a functional obstruction. This means that under the low-pressure circumstances of normal tear drainage, all or part of the lacrimal pathway may collapse. • Jones dye tests may be used to distinguish between patent systems and functionally blocked ones
Primary Jones Test • Instil one drop of fluorescein into the conjunctival sac • Put a cotton bud soaked in anaesthetic in the inferior meatus. • If fluorescein is detected after five minutes, the system is patent (positive Primary Jones Test). • If no fluorescein is discovered, this is a negative Primary Jones Test and the functional obstruction could be anywhere from the punctum to the Valve of Hasner.
Secondary Jones Test • Next, wash the excess fluorescein from the conjunctival sac and syringe. If fluorescein is detected, then this shows it had entered the sac and constitutes a positive Secondary Jones Test and suggests a functional obstruction of the nasolacrimal duct. • If no dye is found on the cotton bud after syringing, this is termed a negative Secondary Jones Test, because fluorescein had not entered the sac and, thus, there is stenosis of the puncta or canalicular system • If no saline appears in the nose, there is a complete obstruction somewhere in the lacrimal drainage system.
Congenital nasolacrimal duct obstructionDiagnosis • Tear meniscus • Dye disappearance test • Irrigation (GA)
Congenital nasolacrimal duct obstruction • Membranous block of the valve of Hasner at the nasal end of the nasolacrimal duct. • Present in 50% of newborns • Clinically evident in 2-6% at 3-4 weeks after birth. • 1/3 bilateral. • 90% resolves in the first year of life.
Congenital nasolacrimal duct obstructionManagement • Massage • Probing +/- Silicone Intubation.
Acquired NLD Obstruction • Hyper secretion (lacrimation) • Impaired drainage (epiphora)
Acquired NLD ObstructionDiagnosis • Irrigation • Dye disappearance test • Johns tests • Scintigraphy • Contrast dacryocystography • CT scan
Acquired NLD ObstructionManagement Dacryocysorhinostomy (DCR)
Dacryocystitis Inflammation of the lacrimal sac secondary to NLD Obstruction.
DacryocystitisManagement • Warm compressors • Oral/ IV broad spectrum antibiotics • Drainage of the abscess • DCR