Download
1 / 22
220 likes | 379 Views
A Therapeutic Platelet Strategy. Journal Club – Feb 21, 2007 Kristine Roland MD FRCPC TM Resident, UBC. Context. Prophylactic plt transfusion strategies for thrombocytopenic pts are standard practice The appropriate plt count ‘trigger’ has evolved:

E N D
A Therapeutic Platelet Strategy Journal Club – Feb 21, 2007 Kristine Roland MD FRCPC TM Resident, UBC
Context • Prophylactic plt transfusion strategies for thrombocytopenic pts are standard practice • The appropriate plt count ‘trigger’ has evolved: - Gaydos et al, NEJM 1962: observed that serious bleeding in pts with acute leukemia rare when plts > 20 x 109/L - Numerous studies indicate threshold of 10 x 109/L is safe: Heckman KD et al, J Clin Oncol 1997 Rebulla P et al, NEJM 1997 Zumberg MS et al, Biol Blood Marrow Transplant 2002 Callow CR et al, Br J Haematol 2002
Context • Does reducing the trigger from 20 to 10 improve plt utilization? - Hersh et al 1998: mathematical modeling predicts a 14.5% decrease in plt utilization - Rebulla 21.5% reduction in plt usage Heckman 35% fewer transfusions (not significant) Callow 36% reduction (compared to retrospective) Zumberg no difference
Context • Other factors impact utilization: frequency of checking plt counts, development of additional risk factors for bleeding, compliance with guidelines • Two studies in the recent issue of Transfusion (Feb 2007) report poorer than expected compliance with prophylactic thresholds: - Greeno et al – overall 28% compliance (up to 43% on Heme/Onc service) - Cameron et al – overall 22% compliance (and reasons for non-compliance were poorly documented)
Context Mark Brecher editorial (Transfusion Feb 2007): • If goal is to reduce plt utilization, other approaches may need to be investigated - Lower plt doses (PLADO study underway) - Employing a therapeutic strategy vs the prophylactic strategy …
The Study: A therapeutic platelet transfusion strategy is safe and feasible in patients after autologous peripheral blood stem cell transplantation Wandt H et al Bone Marrow Transplantation (2006) 37:387-392 • Objective: “ assess the safety and feasibility of a therapeutic platelet transfusion strategy”
Population • Single-centre study from Germany • 106 pts prospectively enrolled after 2001 • Adults undergoing autologous PBSCT - range 18-70 years, median 54 years - male: female 2:1 - MM (43%), lymphoma (32%), acute leukemia (16%), solid tumour (8%) - total of 140 transplant procedures (76 pts received 1 transplant; 30 received 2 or 3) - 87 pts received chemo; 19 pts received chemo +TBI • Exclusion criteria: AL-amyloid, aspergillus infxn, cerebral lesion, prior life-threatening bleeding during chemo
Intervention • daily morning plt counts • twice daily clinical exam for hemorrhage • therapeutic platelet transfusion if bleeding WHO ≥ grade II* • prophylactic platelet transfusion if plt < 10 x 109/Land unstable† • all plts were ABO-compatible apheresis LR • PRBC transfusion to maintain Hb > 80g/L
*WHO Bleeding †Definition of clinically unstable: Fever > 38.5 C Suspicious for aspergillus infection Sepsis Coagulation disorder Planned surgery (goal plt count > 20)
Matched pair analysis • Retrospectively reviewed 60 transplant procedures matched for the first 60 procedures in the prospective cohort • Matched for: gender, Dx, conditioning • These historical patients would have received prophylactic platelet transfusions routinely for morning plt < 10 x 109/L
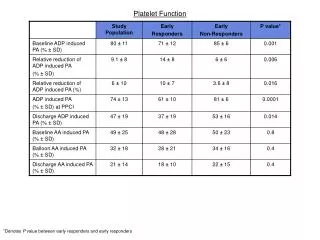
Table 4: Retrospective Analysis Not compared statistically
Of the 140 prospective transplant procedures: - 114 (81%) no bleeding - 28 (20%) WHO grade I - 26 (19%) WHO grade II(mainly epistaxis, mucositis) Of the 60 retrospective matched transplants: - 20% WHO grade II - 1% WHO grade III Results – Bleeding No. of thrombocytopenic days: plts < 20plts < 10 6 (0-92) 3 (0-62)
Results – Transfusions 48 (34%) of 140 transplants could be performed without a plt transfusion. Of the total 235 plt units that were transfused: • 81 therapeutic vs 154 prophylactic - main indications for prophylactic were fever and septicemia - but 27% of transfusions given for no clear reason
Analysis by Dx and conditioning Percentage of transplants (n = 140) NOT requiring platelet transfusion Mann-Whitney U-test TBI associated with increased mucositis-related bleeding
Results – Transfusions Comparison with 60 historical transplants: No statistical analysis Therefore the therapeutic strategy reduced total transfusions by ~50%
Authors’ conclusions • A therapeutic plt transfusion strategy is safe in autologous PBSCT patients - No major bleeding (WHO grade III or IV) - Only 19% minor bleeding (WHO grade II) • A therapeutic strategy reduces the total number of plt transfusions compared to a prophylactic strategy • Pts treated with TBI conditioning regimens more likely to require plt transfusion
Critical Appraisal • Was there randomization? - No; prospective observational cohort (n=140) and a smaller cohort (n=60) of matched historical transplants • Was follow-up complete? - In the prospective cohort, pts followed until plt count > 20 for 2-3 consecutive days - No pts lost after enrolment • Was there blinding? - No; treating physicians needed to be aware of plt transfusion protocol - Bleeding recorded by responsible physician and reviewed by one of the authors (HW or KS)
Critical Appraisal • Were the two groups matched? - First 60 transplants matched for gender, Dx, and TBI conditioning but prospective cohort slightly older (mean 55 vs 49) – no p value given - presumably the two groups were treated similarly except for plt transfusion strategy • Outcomes - Not clear whether all the outcomes reported were predefined at start of study - e.g. # of transfusions related to Dx and conditioning – was this posthoc analysis? Was study powered to detect differences?
Critical Appraisal • Can results be applied to patient care? - Applies to adults undergoing autologous PBSCT - This study used only LR apheresis plts - Pts with prior life-threatening bleeding were excluded, and 34% of all transplants were performed without transfusions – was this a lower risk pt population? • Were all important outcomes considered? - Safety: bleeding complications and number of thrombocytopenic days - no mention of days in hospital or overall mortality - Plt utilization: reduced number of plt transfusions compared to historical controls - significant rate of off-protocol transfusions
ASH 2006: Abstract #577 Oral Session Interim analysis of a prospective randomised study comparing a therapeutic platelet transfusion strategy with the prophylactic platelet transfusion standard in patients after autologous peripheral stem cell transplantation (ASCT). Schaefer-Eckart K, Wendelin K, Wilhelm M, Mahlknecht MU, Conradi R, Schaich M, Leimer L, Wandt H.
Interim Analysis • Prospective randomised study started 2005 • Multicentre • Plan to enrol 200 pts • Prophylactic arm: receive plts if morning plt < 10 • Therapeutic arm: stable pts receive plts only for clinically relevant bleeding • Apheresis or pooled platelet units NS p<0.005
THE END Thank you! Comments and questions …