Download

1 / 17
170 likes | 194 Views
Learn about the poorly understood calcific uremic arteriolopathy, its manifestations, diagnosis, and various treatment options. This report covers the histological findings, epidemiology, triggers, clinical manifestations, and potential therapeutic interventions for this condition.

E N D
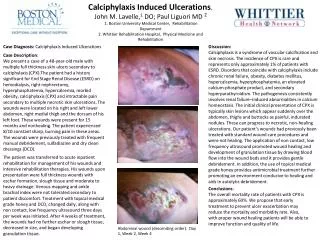
Pathology of “Calcific Uremic Arteriolopathy” • Poorly understood • Systemic medial calcification of arteries that lead to ischemia • Histologically see 1)small vessel mural calcification w or w/o fibrosis (absence vasculitic changes) 2) extravascular calcification 3) vascular thrombosis
Calcium deposition. (A) Hematoxylin-and-eosin staining shows calcifications (purple color) in the walls of arterioles and inflammatory changes in the adipose tissue as a result of ischemia. (B) Calcium deposits can be confirmed by von Kossa's staining, which reveals calcium (black color) in the intima of small- and medium-sized arterioles. Demonstrated here is the characteristic circumferential medial calcific deposit in an arteriole with subintimal edema.
Epidemiology • 1st described in rats 1962 • Most commonly affects those w/ Stage 5 CKD who are on HD and those recently who have recv’d renal transplant • Other reported case reports w/ occurrence in Breast Ca, Alcoholic Liver dz, Chron’s, RA, SLE, Primary Hyperparathyroid
Epi continued…… • True incidence not known, believed to affect 1-4% of pts w/ ESRD • Affects Caucasians >> African Americans • 3 Females :1 Male • One study suggested seen in younger patients w/ history of long duration of HD
Why An Association with ESRD • ?Role of PTH – suggested by beneficial effect of parathyroidectomy = transient uptake of Ca,P (hungry bone) and lower Ca XP product • High doses Vit D induces this in animal models, interesting since analogs like Calcitriol administered to tx 2ndary Hyperparathryoidism in ESRD pts
Other triggers? • Long-term obesity • Recent and sudden weight loss • Malnutrition • Infusion of medications such as iron dextran • Remote and/or recent use of immunosuppressive agents, especially corticosteroids • Liver disease • Diabetes mellitus and insulin injections • Use of vitamin D and calcium-based phosphate binders • Concurrent use of warfarin anticoagulation: Current data suggest that warfarin therapy may lower protein C concentrations, leading to a procoagulant condition in the calcified vessel. Warfarin may also inhibit carboxylation of matrix Gla protein, an important inhibitor of calcification, thus promoting calcification
Clinical Manifestations: • From ischemia one then develops livedo reticularis and/or violaceous painful plaque like subcutaneous nodules where there is most abundant adipose (trunk, buttocks, and proximal extremities)
. The patient in Panel A suffers from end-stage renal disease and has been treated with hemodialysis for more than 4 years. She has had ischemic, nonhealing necrotic ulcerations on her calves for more than 4 months. The patient in Panel B, who was on peritoneal dialysis, presented with a 2-month duration of well-demarcated erythema, hemorrhagic bullae, ulcers, and ecchymoses surrounded by skin thickening and tender subcutaneous indurations.
Clinical Manifestations: • Ulceration is considered a late finding and is associated with a higher mortality rate • Multiple lesions of variable age may be present, following the path of the vasculature. • Less commonly, lesions may manifest as either bullae or distinct subcutaneous, erythematous nodules.
Diagnosis: • Plain films reveal vascular calcifications w/in dermis or subQ tissue (non-specific). ?mammography • Bone Scan can reveal abnormal uptake • Deep Incisional Biopsy** risky • Rule out HyperCoag states and Cryoglbulinemia ~There is no threshold of levels for PTH, Ca, or Phos to exclude/estb this diagnosis
Treatment: • Lower Ca x P product to < 55 w/ non-calcium containing Phosphate binders such as Sevelamer or Lanthanum • Cinacalcet (increases Ca receptor sensitivity to Ca thus normalizing PTH secretion) • Bisphosphonates • ? Role of urgent parathryoidectomy
Pain Management is extremely Important • Surgical c/s for wound care & debridement • Hyperbaric Oxygen therapy has proven successful in several cases
Sodium Thiosulfate – a Novel therapy? • A potent antioxidant that increases solubility of calcium deposits • IV use for calciphylaxis is off-label • Generally well tolerated, but must watch for Anion Gap metabolic Acidosis
~Prognosis • Mortality rate as high as 60-80% in pts w/ ulcerative disease • Most patients succumb to sepsis from their wound infections or organ failure from internal involvement (stone heart) • Location of skin lesions helps predict outcomes: those proximal to elbows/knees (63%) vs distal (23%)
References: Uptodate Cicone JS, Petronis JB, Embert CD, Spector D. Successful treatment of calciphylaxis with intravenous sodium thiosulfate. Am J. Kidney Dis. Jun 2004; 43(6)1104-8. Don BR, Chin AI. A strategy for the treatment of calcific uremic arteriolopathy (calciphylaxis) employing a combination of therapies. Clin Nephrol. 2003;59:463-470. Weenig RH, Sewell LD, Davis MD, et al. Calciphylaxis: natural history, risk factor analysis, and outcome. J Am Acad Dermatol. 2007;56:569-579.