Download
1 / 42
430 likes | 751 Views
Part 3 Sensory Function of the Nervous System. I Sensory pathways. Sensory systems allow us to detect, analyze and respond to our environment “ ascending pathways ” Carry information from sensory receptors to the brain Conscious: reach cerebral cortex

E N D
Part 3 Sensory Function of the Nervous System
I Sensory pathways • Sensory systems allow us to detect, analyze and respond to our environment • “ascending pathways” • Carry information from sensory receptors to the brain • Conscious: reach cerebral cortex • Unconscious: do not reach cerebral cortex • Sensations from body reach the opposite side of the brain
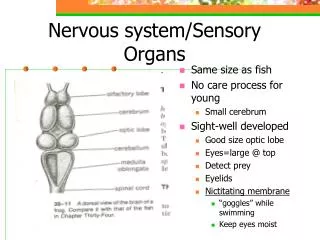
A B C D 1. Sensory receptors A: Free nerve endings (pain, temperature) B: Pacinian corpuscle (pressure) C: Meissner’s corpuscle (touch) D: Muscle spindle (stretch)
Ruffini's endings respond to tension and stretch in the skin
2. Sensory pathways: 3 neurons • 1st: enters spinal cord from periphery • 2nd: crosses over (decussates), ascends in spinal cord to thalamus • 3rd: projects to somatosensory cortex
2.1 Spinothalamic pathway • Carries pain, temperature, touch and pressure signals • 1st neuron enters spinal cord through dorsal root • 2nd neuron crosses over in spinal cord; ascends to thalamus • 3rd neuron projects from thalamus to somatosensory cortex
spinothalamic pathway
Spinothalamic Pathway Primary somatosensory cortex (S1) Thalamus Medulla Small sensory fibres: Pain, temperature, some touch Spinothalamic tract Spinal cord
Left spinal cord injury spinothalamic pathway • Loss of sense of: • Touch • Pain • Warmth/cold • in right leg Spinothalamic damage
2.2 Dorsal column pathway • Carries fine touch, vibration and conscious proprioception signals • 1st neuron enters spinal cord through dorsal root; ascends to medulla (brain stem) • 2nd neuron crosses over in medulla; ascends to thalamus • 3rd neuron projects to somatosensory cortex
dorsal cloumn pathway
Dorsal column pathway Primary somatosensory cortex (S1) in parietal lobe Dorsal column nuclei Thalamus Medulla Medial lemniscus Dorsal column Large sensory nerves: Touch, vibration, two-point discrimination, proprioception Spinal cord
Left spinal cord injury dorsal column pathway • Loss of sense of: • touch • proprioception • vibration • in left leg Dorsal column damage
Dorsal column damage • Sensory ataxia • Patient staggers; cannot perceive position or movement of legs • Visual clues help movement
3.3 Spinocerebellar pathway • Carries unconscious proprioception signals • Receptors in muscles & joints • 1st neuron: enters spinal cord through dorsal root • 2nd neuron: ascends to cerebellum • No 3rd neuron to cortex, hence unconscious
Spinocerebellar tract damage • Cerebellar ataxia • Clumsy movements • Incoordination of the limbs (intention tremor) • Wide-based, reeling gait (ataxia) • Alcoholic intoxication produces similar effects!
4. Somatosensory cortex Located in the postcentral gyrus of the human cerebral cortex.
Spatial orientation of signals. • Each side of the cortex receives sensory information exclusively from the opposite side of the body • (the exception: the same side of the face).
2)The lips, face and thumb are represented by large areas in the somatic cortex, whereas the trunk and lower part of the body, relatively small area. Spatial orientation of signals. 3)The head in the most lateral portion, and the lower body is presented medially
“Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage” International Association for the Study of Pain
Why feel pain? • Gives conscious awareness of tissue damage • Protection: • Remove body from danger • Promote healing by preventing further damage • Avoid noxious stimuli • Elicits behavioural and emotional responses
1. Nociceptors free nerve endings in skin respond to noxious stimuli
Nociceptors • Nociceptors are special receptors that respond only to noxious stimuli and generate nerve impulses which the brain interprets as "pain".
Nociopectors • Adequate Stimulation • Temperature • Mechanical damage • Chemicals (released from damaged tissue) • Bradykinin, serotonin, histamine, K+, acids, acetylcholine, and proteolytic enzymes can excite the chemical type of pain. • Prostaglandins and substance P enhance the sensitivity of pain endings but do not directly excite them.
Hyperalgesia: The skin, joints, or muscles that have already been damaged are unusually sensitive. A light touch to a damaged area may elicit excruciating pain; Primary hyperalgesia occurs within the area of damaged tissue; Secondary hyperalgesia occurs within the tissues surrounding a damaged area.
2. Localization of Pain • Superficial Somatic Pain arises from skin areas • Deep Somatic Pain arises from muscle, joints, tendons & fascia • Visceral Pain arises from receptors in visceral organs • localized damage (cutting) intestines causes no pain • diffuse visceral stimulation can be severe • distension of a bile duct from a gallstone • distension of the ureter from a kidney stone
3. Fast and Slow Pain • Most pain sensation is a combination of the two types of message. • If you prick your finger you first feel a sharp pain which is conducted by the A fibres, • and this is followed by a dull pain conveyed along C fibres.
Fast pain (acute) • occurs rapidly after stimuli (.1 second) • sharp pain like needle puncture or cut • not felt in deeper tissues • larger A nerve fibers • Slow pain (chronic) • begins more slowly & increases in intensity • in both superficial and deeper tissues • smaller C nerve fibers
spinothalamic pathway to reticular formation Aδ nerve C nerve nociceptor nociceptor Impulses transmitted to spinal cord by • Myelinated Aδ nerves: fast pain (80 m/s) • Unmyelinated C nerves: slow pain (0.4 m/s)
somato- sensory cortex thalamus spinothalamic pathway reticular formation Impulses ascend to somatosensory cortex via: • Spinothalamic pathway (fast pain) • Reticular formation (slow pain)
4.Visceral pain Notable features of visceral pain: Often accompanied by strong autonomic and/or somatic reflexes Poorly localized; may be “referred” Mostly caused by distension of hollow organs or ischemia (localized mechanical trauma may be painless)
Afferent innervation of the viscera. Often anatomical separation nociceptive innervation (in sympathetic nerves) from non-nociceptive (predominantly in vagus). Many visceral afferents are specialized nociceptors, as in other tissues small (Ad and C) fibers involved. Large numbers of silent/sleeping nociceptors, awakened by inflammation. Nociceptor sensitization well developed in all visceral nociceptors.
Referred pain • Pain originating from organs perceived as coming from skin • Site of pain may be distant from organ
Convergence theory: This type of referred pain occurs because both visceral and somatic afferents often converge on the same interneurons in the pain pathways. Excitation of the somatic afferent fibers is the more usual source of afferent discharge, so we “refer” the location of visceral receptor activation to the somatic source even though in the case of visceral pain. The perception is incorrect. Referred pain The convergence of nociceptor input from the viscera and the skin.
5. “Pain Gate” Theory Melzack & Wall (1965) A gate, where pain impulses can be “gated” The synaptic junctions between the peripheral nociceptor fiber and the dorsal horn cells in the spinal cord are the sites of considerable plasticity. A “gate” can stop pain signals arriving at the spinal cord from being passed to the brain • Reduced pain sensation • Natural pain relief (analgesia)
descending nerve fibers from brain axons from touch receptors pain pathways axons from nociceptors “THE PAIN GATE” opioid-releasing interneuron
How does “pain gate” work? The gate = spinal cord interneurons that release opioids. The gate can be activated by: • Simultaneous activity in other sensory (touch) neurons • Descending nerve fibers from brain
Applications of pain gate Stimulation of touch fibres for pain relief: • TENS (transcutaneous electrical nerve stimulation) • Acupuncture • Massage Release of natural opioids • Hypnosis • Natural childbirth techniques
6. Pain Relief • Aspirin and ibuprofen block formation of prostaglandins that stimulate nociceptors • Novocain blocks conduction of nerve impulses along pain fibers • Morphine lessen the perception of pain in the brain.