Download
1 / 39
390 likes | 650 Views
Retinal Anatomy. Posterior Vitreous Detachment (PVD). Vit: collagen+ hyaluronic acid (mucopolysaccharide) Loss of gel contractile force defect in posterior vit. Face liquid escape posteriorly exam: Biomicroscopic, B-scan ultrasonography, OCT Autopsy study:

E N D
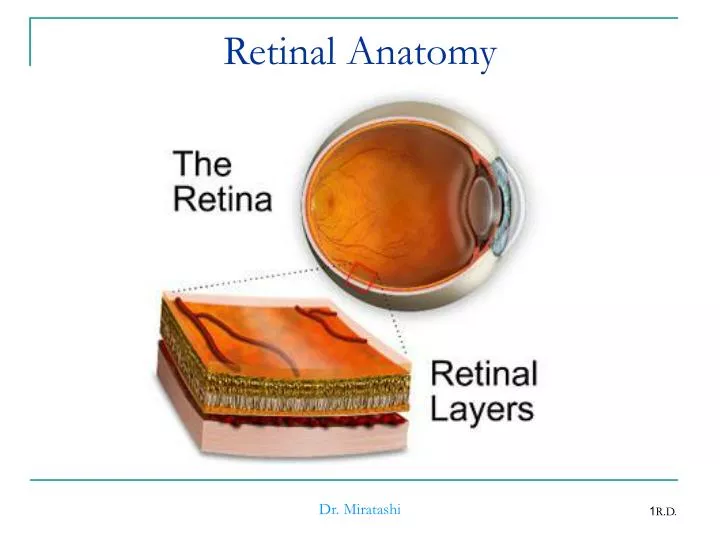
Retinal Anatomy Dr. Miratashi
Posterior Vitreous Detachment(PVD) • Vit: collagen+ hyaluronic acid (mucopolysaccharide) • Loss of gel contractile force defect in posterior vit. Face liquid escape posteriorly • exam: • Biomicroscopic, B-scan ultrasonography, OCT • Autopsy study: • <10% under age of 50years but 63%over age of 70 Dr. Miratashi
P.V.D. • Patient’s age • Aphakia • Inflammatory disease • Trauma • Myopia Dr. Miratashi
Symptoms of PVD • Flashing lights • Floaters • Acute PVD have 15% netinal tear • PVD with vit. Hemorrhage 50%-70% have retinal tears • PVD without vit. Hemorrhage 10%-12% have retinal tears Dr. Miratashi
PVD and Cataract Surgery • 66% - 100% PVD • ICCE 84% • ECCE with open capsule 76% • ECCE intact capsule 40% Dr. Miratashi
Retinal Breaks • Full-thickness defect in the neurosensory retina • Provide access for liquid to enter potential space between sensory retina & RPE • Flap or horseshoe tear • Giant retinal tear 90 or more • Operculated hole • Dialysis (ora serrata) • Atrophic retinal hole (no traction not R.D) • Macular hole Dr. Miratashi
Trauma In Eyes • 12% are found immediately • 30% are found within 1 month • 50% are found within 8 months • 80% are found within 24 months Dr. Miratashi
Lattice Degeneration • 6%-10% of general population • Is bilateral in1/3-1/2 of affected patients • More in myopic eyes • Familial predilection • Small number of lattice develop R.D. • But 20%-30% of R.D. have lattice Dr. Miratashi
Histopathology of Lattice • Discontinuity of I.L.M. • Liquified vitreous • Atrophy of inner layers of retina • Condensation and adherence of vitreous at the margin Dr. Miratashi
Aphakia and Psuedophakia • 1%-3% have risk of R.D. compare to phakic • Should be warned of potential symptoms Dr. Miratashi
Fellow eye in patient with R.D. • 10% of phakic 20%-36% of aphakic will develop R.D. in second eye • An other risk factor is present prophylactic treatment Dr. Miratashi
Horseshoe tears Dialysis Operculated tear Atrophic hole Lattice degeneration without horseshoe tears Almost always Almost always Sometimes Rarely Rarely Indication for Treat of retinal tears and holes in symptomatic patients Dr. Miratashi
Sub Clinical R.D. • Asymptomatic R.D. • Fluid extends more than 1DD from the break but not more than 2DD posterior to the equator • 30%will progress to R.D. so treat is recommended Dr. Miratashi
Retinal Detachment • Rhegmatogenous, most common, rhegma means break • Tractional less common • Exudative or secondary Dr. Miratashi
Symptom and Sign of R.D. • Photopsia or floater • vision • Visual field defect • IOP • Shafer’s sign (tobacco dust) in vitreous or anterior segment • Corrugated appearance • In long standing R.D. P.V.D., fixed folds Dr. Miratashi
Management of R.R.D. • Find all breaks • Create a chorioretinal irritation around each break • Laser • Cryo • Diathermy • Bring the retinal and choroid into contact to close the break • Scleral buckle, pneumatic retinopexy for superior break • Vitrectomy in selected cases Dr. Miratashi
Anatomic Reattachment • Overall rate is 90% • Aphakia and psuedophokia less prognosis • Giant tear, PVR, uveitis, choroidal detachment • Posterior break has worst prognosis Dr. Miratashi
P.V.R. • Cause of failure to repair • RPE., glial, other cells an inner and outer retinal surface forming membrane • Contraction fixed fold, new break, reopen old break A, B, C, anterior, posterior Dr. Miratashi
Post Operative Vision • The status of macula • 1week macula detach. 75% obtain 20/70 or better • 1-8 weeks 50% same vision • Even with on macula preoperatively post operation may develop macular edema or pucker • Intra operative complication may also limit visual recovery Dr. Miratashi