Download
1 / 32
320 likes | 526 Views
NERVE-ROOT PAIN. Outcomes. Be familiar with the pathology of a typical nerve root pain. Be familiar with the causes of nerve root symptoms. Be familiar with the clinical presentation of nerve root irritation, nerve-root pressure, pressure on

E N D
Outcomes Be familiar with the pathology of a typical nerve root pain. Be familiar with the causes of nerve root symptoms. Be familiar with the clinical presentation of nerve root irritation, nerve-root pressure, pressure on the spinal cord and pressure on the caudaequina. Be familiar with the distinct characteristics of nerve root pain.
Outcomes Be familiar with the most widely used physiotherapy treatment protocol for a patient with a typical severe nerve root pain. Be familiar with the most widely used physiotherapy treatment protocol for a patient with a cervical, lumbar, chronic and intermittent nerve root pain. Be familiar with the clinical presentation of a typical patient with nerve root pain.
Outcomes Be familiar with the deep spinal muscles that can simulate nerve root symptoms.
Nerve-root pain Pressure on the nerve-root causes pain The pain does not come form the nerve-root itself, but develops as a results of venous congestion The first sign is pins and needles in the distal region of the affected dermatome The pain intensifies and the arterial blood circulation is restricted The nerve’s conduction is suspended and signs of nerve-fall out develops
Degree of impairment Strength of the initial impulse Duration of the abnormal pressure (the longer the worse it becomes)
Causes Disc prolapse Disc protrusion Osteophytes Traction injuries Swelling in the intervertebral canal and foramen Relaxed ligamentumflavum Hypertrophic capsule
Causes Stenosis Adhesions Deep-seated muscle spasm / trigger points Instability of the movement segment
Nerve-root irritation Increased reflexes Paraesthesia / abnormal sensation
Nerve-root compression Decreased reflexes Loss of sensation or no sensation Muscle weakness – long-term muscle atrophy
Pressure on the spinal cord Gait disturbances / clumsiness Bilateral pins and needles Bladder dysfunction Increased reflexes below the level of the lesion + clonus + Babinski
Pressure on CaudaEquina Saddle anaesthesia Urine retension
Characteristics of nerve-root pain Area Nature Movement Deformities
Area Well defined throughout the dermatome or Dominates the distal part of the dermatome Can occur in regions of the dermatome
Nature Severe pain – the patient appears to be experiencing a lot of pain, sometimes a total loss of function Pain may be latent, often undulant and builds up Sometimes a sharp, shooting pain that paralyses the patient In acute phase the pain is constant and severe In sub-acute and chronic phase the pain is intermittent
Latent pain Worsens after activities Worse towards the end of the day Worsens during sustained positions
Cloward Areas Imminent nerve-root pain of C7 refers to the medial border of the scapulae with cervical movements S1 refers pain deep to the medial buttocks
Movement Examination will reveal that movements either causes distal pain or latent pain in the distal segment The more distal pain is caused, the more carefully a patient needs to be managed
Deformities Protective deformities occur Patient stands on one leg with the other leg bent and toes resting on the floor
Generalised treatment Severe nerve root pain is difficult to treat Patients respond slowly Pain takes long to disappear It takes about 2 weeks before any improvement can be observed
Severe nerve root pain Hospital or traction as an outpatient Neurological examination is a ABSOLUTE PRE- REQUISITE for traction Immediate TOTAL relief must not be achieved with traction under any circumstances If total relief is obtained if may also cause severe sharpening of symptoms Traction takes approximately 4 days to show an effect and the initial effect may be minimal Palpation techniques are a contra-indication
Severe nerve root pain As soon as the symptoms improve mobilisation techniques namely Grade Gr IV- may be added to traction Treated daily for 3 weeks Thereafter intermittent for 6 weeks Treatment is suspended after 85% improvement If a plateau is reached after 2 weeks of treatment, the treatment must be suspended, in order to give the treatment pain time to subsided
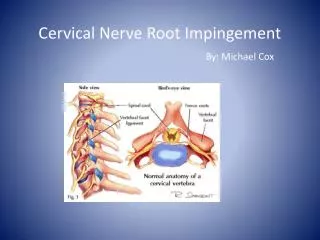
Specific treatment Cervical nerve root pain Neurological evaluation Constant traction Collar for support to restrict movement – wean as soon as possible Advice regarding sleeping position (mid position) Later rotation and longitudinal In the case of OA add central and unilateral PA’s
Specific treatment Lumbar nerve root pain Neurological evaluation Total bed rest Constant traction Advice Later rotation and direct mobilisations with OA Takes longer to react to treatment
Chronic nerve root pain History of prolonged pain in the back and leg No specific incident
Chronic nerve root pain Signs Prolonged history Slow progress Reasonably stable condition Symptoms vary very little Activities make very little difference to the pain
Chronic nerve root pain Objective Sometimes no comparable sign Make use of differentiation tests Movements at end of range sometimes causes local back pain No latent pain Sustained positions (especially quadrant) sometimes positive
Chronic nerve root pain Treatment Treatment by means of strong techniques Add one technique daily Traction and SLR Little reaction to traction SLR works well Manage in much the same manner as OA patients
Chronic nerve root pain Deep spinal muscles: m quadratuslumborum m serratus post inf m piriformis m quadratusfemoris can simulate nerve root pain symptoms – always give attention to these muscles during treatment
Intermittent nerve root pain Pain often occurs in only one dermatome Long-term problem Local hypertrophy and palpation tenderness of the interspinal ligament Movements appear stiff Quick active tests and palpation techniques do not reproduce the symptoms
Intermittent nerve root pain Treatment Palpation techniques initially Trigger points Neural mobilisation Cross-frictions Ultrasound to treat the hypertrophic ligament “Dry needling”