Download
1 / 19
190 likes | 213 Views
Learn about a comprehensive project enhancing TB services for nomadic populations in North-Eastern Nigeria. Discover the background, objectives, strategies, interventions, results, challenges, and lessons learned. Explore the project's impact on TB case notifications and treatment outcomes amidst unique challenges faced in screening and linking nomads to care. Gain insights into the key strategies and lessons learned for sustainable community health initiatives.

E N D
TB Screening & Linkage to Care for Nomadic Populations in North-Eastern Nigeria The 49th Union World Conference on Lung Health, The Hague, October 2018 Stephen John, MD, MPH/ICHD (CEO, Janna Health Foundation)
Outline • Overview of the Project: • Background • Objectives • Strategies • Key Interventions • Results • Challenges in TB Screening & Linkage to Care • Lesson Learnt • Conclusion
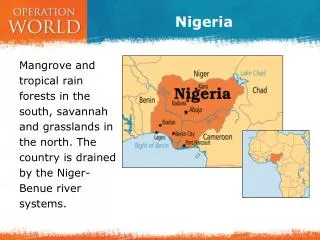
Project Location & TB Services • Population: 3.8 m • Land Mass: 42,000 Km2 • Number of BMUs: 21 • Total Health Facilities: 1,040 • Total DOTS Centers: 142 • Coverage: 1/27,000 pop • TB Diagnostic Centers: • GeneXpert: 1 • AFB Microscopy: 44 • Coverage: 1/87,000 pop • Target Population: 0.45 m • Evaluation Population: 3.8 m Map of Nigeria and Adamawa State
Background..1 • Over 50m Nomads Globally: • 30m (60%) in Africa • Estimated 9.3m Nomads in Nigeria: • 5.3m are Nomadic Pastoralists • Estimated 450,000 in Adamawa • 4m are Nomadic farmers/fishermen • High Rates of TB among Nomads: • Sahelian Nomads, • Maasai, Fulani & other Nomads in Africa Chabasse et al, 1985, Omar, 1992, Van Cleeff et al, 1995, A. Sheik-Mohammed & J. P. Valema 1999
Background…2 • Factors influencing high rates of TB: • Poor access to Health Facilities • Malnutrition • Poor Housing (overcrowding/ventilation) • Consumption of un-pasteurized milk • High rates of Bovine TB • Mobile population • Poor vaccine coverage (BCG) • Low level of formal education/Low awareness on TB • Low Literacy rate of (0.2 – 2%) Imperato, 1975; Ailou, 1992, Omar, 1992, E. F. Ejeh et al, 2013, Adamu et al, 2015; Ige. M. Tilo et al, 2017
Objectives • To expand TB services in an innovative and highly collaborativemanner through the involvement of the Nomadic Leaders to ensure communityownershipandsustainability • To determine whether or not the incidence rates of TB among the target population is higher as compared to the evaluation population
Key Strategy: Preparatory..1 • Identification, orientation & linkage of “Contact” Person with the TB Programme (State & LGA levels) • Mapping: • Grazing Reserves, Nomadic settlements, Resting Points & Health Facilities (proximal to reserve, route & resting points) • Identification & engagement of Nomadic Community Leaders • Advocacy Meeting with Community Leaders • Identification/Selection of CVs & HCWs
Key Strategy: Preparatory..2 • Training/orientation of CVs, HWs & Lab Staff • Develop/pre-test jingles in “Fulfulde”, “Hausa” and English • Re-constitute ACSM Committee • Advocate to line Ministries/Boards: • Ministry of Health, LGAs, Livestock Production & Universal Basic Education Board (UBEB)
Interventions • ACSM: • Strategic & sustained advocacy to key stakeholders including result sharing • Broadcast of Radio & TV Jingles • Active TB Case Finding: • Tent-to-tent screening of settlements • Outreach on Market days • Sputum transportation & Diagnosis: • AFB Sputum Microscopy • GeneXpert for SS- presumptives • Linkage to care
Impact of ACF on TB Case Notifications: ‘08 –’17 TB REACH Insurgency
Impact of ACF onAdamawa’s TB Treatment Outcomes Cured Treatment Completed Died Treatment Failure Loss to Follow-up Transfer Out Despite more people being treated in 2012, outcomes were better than 2011.
Challenges in TB Screening/Linkage to Care..1 • No appropriate guidelines/SOPs: • NTP to develop appropriate guidelines for their key populations • Maps of cattle routes: • Need for validation • Engagement process: • Peculiarity of Nomadic Communities • Difficult topography/Hard-to-Reach • Appropriate project vehicles • Strategic decentralization of TB services
Challenges in TB Screening/Linkage to Care..2 • Climatic Condition: • Schedule more activities in the dry season • Childhood TB Diagnosis • Delays in commencement of treatment • Replacement Worker • Migration • Alternative TB Care: • Traditional Healers, PMVs and CPs • Adherence to TB Treatment • Community Leader engagement/involvement • PARE Trained HCWs & Nomadic CVs/TS • Language Barrier!
Lesson Learnt • Dealing with a mobile population • TB Screening: Target market days, resting points, cattle routes & grazing reserves • Treatment/adherence: Use Nomadic youth as CVs and sustained engagement of Community Leaders • Communication: LGA TB Supervisors, HCWs, sustained supplies • Use of Veterinary Dispensaries for DOTS • Use of Nomads as CVs • Cross border interventions • Strategic advocacy and result sharing • Ownership & Sustainability
Acknowledgements • Adamawa & Taraba State Governments • The 2 State TB Programme Teams • Pastoral Resolve (PARE); Adamawa State • KNCV Nigeria • NTBLCP, Nigeria • Netherlands Leprosy Relief • Members of the Global indigenous STOP TB initiative (GISI) Funders • TB REACH / Stop TB Partnership • Global Affairs Canada