Download
1 / 116
1.4k likes | 3.55k Views
ECG Interpretation. Advanced Cardiac Life Support. William A. Shapiro, M.D. http://anesthesia.ucsf.edu/shapiro. advancing health worldwide TM. Department of Anesthesia and Perioperative Care. Course Objectives & Description:.

E N D
ECG Interpretation Advanced Cardiac Life Support William A. Shapiro, M.D. http://anesthesia.ucsf.edu/shapiro advancing health worldwide TM Department of Anesthesia and Perioperative Care
Course Objectives & Description: • Recognize & initiate early management of peri-arrest conditions that may result in cardiac arrest • Manage cardiac arrest until return of spontaneous circulation, or transfer of care • Understanding of arrhythmia interpretation • Recognize the hemodynamic consequencesof arrhythmias
Normal Sinus Rhythm Normal sinus rhythm results from the initiation of an electrical signal (the cardiac impulse) by cells of the sinus node at a rate appropriate to the age and state of activity of the individual, and then the propagation of that signal in an orderly manner through the atria, A-V junction, ventricular specialized conducting system and the ventricular myocardium
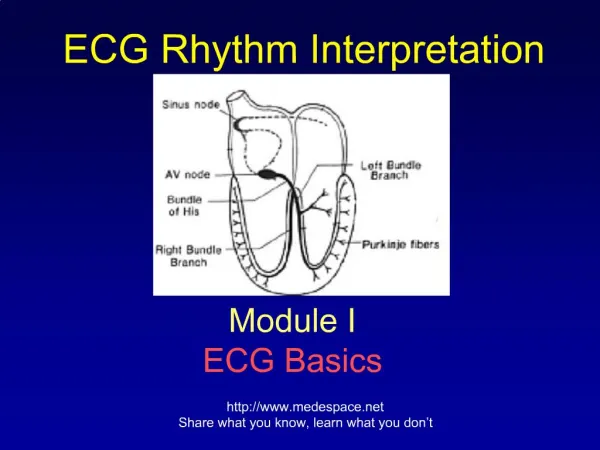
Cardiac Conduction System Bachmann’s bundle Sinus node Internodal pathways Left bundle branch AV node Posterior division Bundle of His Anterior division Purkinje fibers Right bundle branch
Arrhythmia An arrhythmia reflects either abnormally rapid or slow impulse initiation by the sinus node, or interruption of the sinus rhythm by impulses originating from some other site in the heart, either for short or long periods of time
Mechanisms of Arrhythmias • Reentry • Automaticity • Altered normal automaticity • Abnormal automaticity • Triggered Rhythms due to DAD (delayed after depolarizations
Causes of Arrhythmias • Physiologic and Pathologic Processes • Vagal stimulation, Fever, Hypothermia • Electrolyte abnormalities, CNS problems • Hypovolemia, Pain, anaphylaxis, etc. • Preexisting Cardiac & Pulmonary Disease • Acute coronary syndrome, HTN, AODM • COPD, hypoxia, hypercarbia
The Electrocardiogram R T P U Q S PR Interval QRS Interval
The Electrocardiogram PR Interval QRS Interval QT Interval
Cardiac Conduction System Relationship of ECG to anatomy
Cardiac Conduction System Relationship of ECG to anatomy
ACLS THE ACLS PROVIDER IS: IN
Normal Sinus Rhythm • Rate 60-100 beats per minute • Rhythm: Regular • P waves: Upright in Leads: 1, 2, AVF
Sinus Tachycardia • Rate: Greater than 100 beats per minute • Rhythm: Regular • P waves: Upright in Leads: 1, 2, AVF
Sinus Tachycardia • Rate: Greater than 100 beats per minute • Rhythm: Regular • P waves: Upright in Leads: 1, 2, AVF
Sinus Bradycardia • Rate: Less than 60 beats per minute • Rhythm: Regular • P waves: Upright in Leads: 1, 2, AVF
Sinus Bradycardia • Rate: Less than 60 beats per minute • Rhythm: Regular • P waves: Upright in Leads: 1, 2, AVF
Premature Atrial Complexes • P wave Rhythm: Irregular • P waves: Premature, often in the T-wave • QRS complex: Normal or widened P-wave
Premature Atrial Complexes • P wave Rhythm: Irregular • P waves: Premature, often in the T-wave • QRS complex: Normal or widened
Premature Atrial Complexes • P wave Rhythm: Irregular • P waves: Premature, often in the T-wave • QRS complex: (Normal or widened) or blocked Non conducted P-wave
Atrial Tachycardia • Rate: Atrial- 140-240 bpm, p-waves hard to see • Rhythm: • P-wave- regular • QRS- 1-1 conduction with atrial rates < 200 bpm • With atrial rates > 200 bpm, A-V conduction block common (less than 1-1 conduction) • PR interval- depends on the origin of the p-wave • QRS- usually normal
P-Wave P-Wave Atrial Tachycardia
Atrial Tachycardia Atrial Tachycardia with variable block P-Waves are regular at 160 bpm
Atrial Flutter • Rate: Atrial- 300 bpm (260-320) • Rhythm: • P-waves- regular • QRS- 2-1 conduction - 150 bpm, variable AV conduction with constant AV conduction ratio • P-waves: F-waves (Flutter), sawtooth pattern • QRS- usually normal, obviously sometimes wide
Atrial Flutter F-waves
Atrial Flutter Atrial Flutter with variable conduction (block)
Atrial Fibrillation • Rate: Atrial- rapid, Ventricular- Depends • Rhythm: • P-waves- irregular • QRS- beat to beat variability, Irregularly irregular • P-waves: From F-waves (Flutter) to absent • QRS duration- normal or wide
Premature Junctional Complexes • Rhythm: Irregular • P waves: Retrograde • PR interval: < .12 sec or nonexistent • QRS complex: Normal or widened
Premature Ventricular Complexes • Rhythm: Irregular • P waves: Usually not seen • QRS complex: Wide > .12 sec • Compensatory pause
This is the sinus and the QRSdistance This distanceis double the sinus distance Premature Ventricular Complexes Compensatory pause
Premature Ventricular Complexes • Unifocal PVCs • Multifocal PVCs
This is the sinus and the QRSdistance This distanceis double the sinus distance Premature Ventricular Complexes Compensatory pause Interpolated PVC
Premature Ventricular Complexes Ventricular Bigeminy Pairs of PVCs
Premature Ventricular Complexes PVC on T-wave precipitating Ventricular Tachycardia
Ventricular Tachycardia • Rate: Approx 100-230 bpm • Rhythm: Usually regular • P waves: Usually not seen • Independent A and V activity • A-V dissociation • QRS complex: Wide > .12 sec • Capture beats, fusion beats
Ventricular Tachycardia Polymorphic Ventricular Tachycardia
Ventricular Fibrillation • Rate: Rapid- no effective cardiac rhythm • Rhythm: Irregular • P, QRS, T- waves: Absent • No blood pressure!
Ventricular Fibrillation Course VF Fine VF
Ventricular Asystole • P, QRS, T- waves: Complete absent of cardiac electrical activity • Complete absent of effective cardiac pumping function